Punch biopsy is central to diagnostic decision-making, as inadequate depth or distorted architecture can lead to incomplete evaluation and may necessitate repeat procedures.
For this reason, both punch size and technique play a critical role in determining sample reliability.
Variations in diameter, depth, and specimen handling can affect diagnostic accuracy, particularly in inflammatory dermatoses or lesions requiring architectural assessment.
Although smaller punches such as 2.5 mm may be appropriate in selected cases, achieving sufficient depth remains essential for comprehensive analysis.
You’ll learn the key factors surgeons consider when choosing the most appropriate punch biopsy tools, including size, anatomical site, and technique.
Key Takeaways:
- Punch biopsy tools provide controlled full-thickness sampling, enabling accurate evaluation of skin architecture for histopathologic diagnosis.
- Punch size selection directly impacts diagnostic yield and the need for closure, requiring a balance between tissue adequacy and cosmetic outcome.
- A 4 mm punch is most commonly used as it offers sufficient tissue for most conditions while maintaining acceptable healing outcomes.
- Larger punches (5–6 mm) are used when deeper sampling or additional studies are required, improving diagnostic reliability in complex cases.
- Technique and anatomical location together determine specimen quality and healing, influencing both depth control and closure decisions.
What Are Punch Biopsy Tools?
Punch biopsy tools are used when diagnostic accuracy depends on obtaining a full-thickness skin specimen with preserved architecture. These cylindrical instruments remove samples, including the epidermis, dermis, and, depending on insertion depth and site, superficial subcutaneous tissue.
Each punch features a hollow, sharp circular blade attached to a pencil-like handle, allowing precise vertical insertion with controlled rotation for consistent sampling and minimal tissue distortion.
A clear definition of punch biopsy tools makes it easier to examine the variations in type and size used in current practice.
Different Types & Sizes of Punch Biopsy Tools in 2026
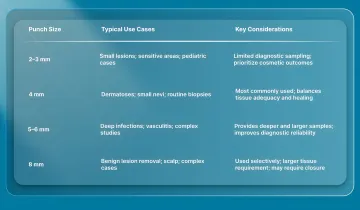
Punch biopsy tools typically range from 2 mm to 8 mm, with each size suited to specific clinical scenarios. Below are the different types, typical uses, and selection considerations.
1. 2mm and 3mm Punches
These smaller punches are typically used in situations where tissue preservation and cosmetic outcome are priorities, particularly in visible or anatomically sensitive areas.
- Small lesions in cosmetically sensitive areas such as the face, hands, and neck
- Pediatric patients requiring minimal tissue disruption
- Situations where minimizing scarring is a priority
- Limited diagnostic sampling when a smaller specimen is expected to be sufficient
2. 4mm Punches
The 4 mm punch is the most commonly used size in clinical practice, providing a balance between specimen adequacy and acceptable cosmetic outcome.
- Most inflammatory dermatoses, including eczema, psoriasis, and lichen planus
- Small nevi requiring diagnostic evaluation
- Routine diagnostic biopsies across a range of anatomical sites
- Conditions where preservation of full-thickness skin architecture is necessary
3. 5mm and 6mm Punches
Larger punches are selected when greater tissue volume or deeper sampling is required to support diagnosis.
- Suspected deep infections, including panniculitis and deep fungal infections
- Inflammatory conditions requiring assessment of subcutaneous tissue
- Cases requiring multiple diagnostic studies, including histology and immunofluorescence
- Vasculitis, where adequate vessel sampling is necessary
4. 8mm Punches
The largest commonly used punches are reserved for selected diagnostic and therapeutic situations where a larger specimen is required.
- Complete removal of small benign lesions when size and location permit
- Excision of nevi in non-cosmetically sensitive areas such as the trunk or proximal extremities
- Cases requiring larger tissue samples for multiple or complex diagnostic tests
- Scalp biopsy for alopecia, where two 4 mm punches are often preferred for optimal sectioning
In cases where closure extends beyond simple suturing, bioabsorbable subcuticular systems such as SubQ It! SU-10 may be considered for small-incision procedures.
These systems approximate tissue beneath the skin surface, eliminating the need for staple removal and aligning with efforts to reduce follow-up requirements and improve procedural efficiency.
Once the available types and sizes are understood, selecting the right punch biopsy tool requires careful consideration of several practical factors.
5 Key Factors to Consider While Choosing the Right Punch Biopsy Tools
Selecting the right punch size affects diagnostic yield, specimen adequacy, and closure planning. Surgeons aim to obtain enough tissue for accurate histopathology while minimizing excess removal, scarring, and procedural complexity.
Size choice should consider lesion characteristics, diagnostic goals, anatomy, and downstream management. The following factors outline practical decision-making.
1. Lesion Size and Characteristics
Punch diameter should be matched to the lesion’s size, morphology, and diagnostic objective, rather than using a single standard size across all cases.
2. Anatomical Location
Anatomical site influences punch size, depth, and closure planning, affecting both diagnostic adequacy and cosmetic outcomes. Surgeons consider regional skin thickness, vascularity, and tension when choosing instruments and techniques.
Punch selection should be tailored to each body site, as outlined below.
Site-specific considerations include:
- Face and cosmetically sensitive areas: Smaller punches are generally preferred due to higher cosmetic priority and the ability of well-vascularized areas to heal effectively.
- Thin dermis regions (eyelids, ears, genitals): These areas require careful depth control regardless of punch size to avoid excessive penetration due to thinner dermal layers.
- Trunk and extremities (4–8 mm): Larger punches are better tolerated in these areas, where thicker dermis allows for more substantial specimens, and closure with sutures is more feasible.
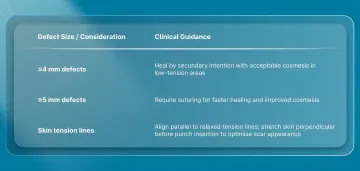
3. Healing and Cosmetic Considerations
Healing outcomes after punch biopsy are influenced by defect size, anatomical location, and skin tension, all of which affect whether closure is required.
The following patterns are generally observed in practice:
4. Specimen Adequacy for Pathologic Evaluation
Beyond technique and location, punch size must ensure that the specimen is adequate for histopathologic interpretation, particularly when diagnosis depends on architectural detail.
Key requirements include:
- Sufficient tissue for multiple histologic sections
- Preservation of tissue architecture without a crush artifact
- Adequate depth for evaluation of dermal and subcutaneous involvement when required
- Enough material to support additional studies, including special stains or immunohistochemistry
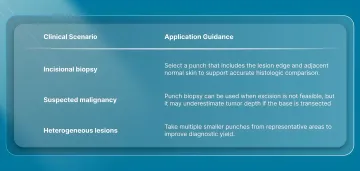
Providing the pathologist with a clear clinical differential diagnosis further improves diagnostic accuracy by guiding tissue evaluation.
5. Cost and Availability
Instrument selection is also influenced by practical considerations related to workflow, consistency, and resource management.
- Disposable vs reusable tools: Disposable punch biopsies are single-use, sterile, and maintain consistent sharpness without reprocessing. Reusable tools require sterilization and may dull over time, affecting specimen quality.
- Stocking strategy: Maintaining a standard set of sizes allows surgeons to address a wide range of diagnostic scenarios without procedural delays.
- Cost-effectiveness: Appropriate punch selection reduces the likelihood of inadequate sampling and repeat procedures, thereby reducing clinical burden and overall cost.
Beyond selecting the right tool, proper technique plays an equally important role in achieving reliable biopsy outcomes.
A Checklist to Complete Proper Punch Biopsy Technique
The technique directly determines whether a punch biopsy yields a diagnostically adequate specimen without artifacts or complications. A structured approach, from preparation through specimen handling, helps standardize outcomes across cases.
Here’s a checklist for a proper punch biopsy procedure:
Pre-procedure:
- Obtain informed consent, including discussion of risks, benefits, and expected outcomes
- Review patient medications, particularly anticoagulants, antiplatelet agents, and immunosuppressants
- Prepare the site using an antiseptic solution such as chlorhexidine or povidone-iodine
- Infiltrate the area with local anesthetic using the intradermal technique
Anesthesia:
- 1% lidocaine is most commonly used for punch biopsy procedures
- Addition of epinephrine (1/100,000) improves hemostasis and prolongs anesthetic effect; its use in digits, nose, and ears is considered safe in appropriate clinical settings
- Buffering with 1:9 bicarbonate may reduce injection discomfort
- Allow adequate time for the anesthetic effect before proceeding
Biopsy procedure:
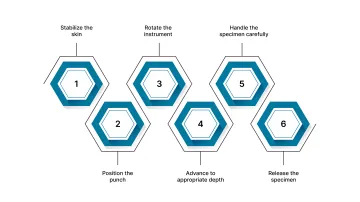
- Stabilize the skin: Apply gentle traction perpendicular to relaxed skin tension lines so the circular defect relaxes into an elliptical shape, facilitating closure
- Position the punch: Hold perpendicular to the skin surface with steady downward pressure
- Rotate the instrument: Use a controlled back-and-forth twisting motion rather than continuous rotation
- Advance to appropriate depth: Continue until a decrease in resistance indicates entry into the superficial subcutaneous layer
- Handle the specimen carefully: Elevate using a needle or skin hook to avoid crush artifact; avoid toothed forceps
- Release the specimen: Use fine scissors to sever the base at the subcutaneous level
Post-procedure:
- Achieve hemostasis using direct pressure, topical agents such as aluminum chloride, or light electrocautery when needed
- Select a closure method based on punch size, anatomical location, and skin tension
- Apply an appropriate dressing and provide wound care instructions
- Submit the specimen in formalin or an appropriate transport medium when specialized studies (e.g., immunofluorescence) are required.
Final Thoughts
Choosing the right biopsy punch influences more than just specimen quality. It affects healing, follow-up requirements, and overall procedural efficiency.
As procedural demands change, there is growing interest in closure approaches that minimize additional steps while maintaining precise tissue approximation.
In this context, SubQ It! SU-10 offers a bioabsorbable subcuticular closure system designed for small surgical incisions, placing fasteners beneath the skin to approximate wound edges without external penetration.
Because the fasteners are bioabsorbable, there is no requirement for a follow-up visit for removal, supporting both workflow efficiency and patient convenience.
Contact us to explore how SubQ It! SU-10 can support closure in small-incision procedures and improve procedural efficiency.
FAQs
1. What is the difference between a punch biopsy and a shave biopsy?
A punch biopsy removes a full-thickness cylindrical sample of skin, while a shave biopsy removes only superficial layers. You would use a punch biopsy when architectural detail is needed, but for suspected melanoma, an excisional biopsy is preferred when feasible.
2. What size punch biopsy tool should I use for different types of skin lesions?
In most cases, a 4 mm punch is sufficient for inflammatory conditions and routine biopsies. For deeper or more complex cases, a 5–6 mm punch may be needed; for small benign lesions, a 1–2 mm punch is sufficient.
3. How deep should a punch biopsy go?
You should advance the punch through the dermis into the superficial subcutaneous layer to obtain an adequate sample. The depth should be adjusted based on the anatomical site, especially in thinner areas.
4. Do I need to suture a punch biopsy site?
Small punch biopsy defects, typically ≤3–4 mm, can often heal without sutures, especially in low-tension areas. Larger defects or sites under higher tension generally require suturing to ensure proper wound closure and healing.
5. Can I reuse punch biopsy tools?
Most modern punch biopsy tools are single-use to maintain sharpness and reduce the risk of infection. Reusable tools can be used if properly sterilized, but they may lose cutting efficiency over time.
6. What is the best punch biopsy technique for suspected melanoma?
You should perform a complete excisional biopsy with a scalpel whenever possible to allow accurate staging. If that is not feasible, a punch biopsy from a representative area may be used, but it can underestimate tumor depth.
7. How long does it take for a punch biopsy to heal?
Healing time varies based on size, depth, and location. Small punch biopsies typically heal within 7-10 days, while larger or sutured sites may take longer, with complete healing continuing over several weeks.
8. What is a cervical biopsy tool and its types?
A cervical biopsy tool is used to remove tissue from the cervix for diagnostic evaluation. Common types include punch biopsy forceps, endocervical curettes (ECC), and excisional methods such as LEEP or cone biopsy, each suited to different depths and clinical indications.
9. What are the biopsy needle types and their advantages?
Biopsy needles include fine-needle aspiration (FNA), core needle biopsy (CNB), and vacuum-assisted biopsy (VAB). They enable minimally invasive tissue sampling, are typically faster than surgical biopsy, and often avoid open procedures.
10. What are the limitations of biopsy needles and their side effects?
Biopsy needles may provide limited or non-representative samples, which can affect diagnostic accuracy. Common side effects include bleeding, pain, and bruising, as well as a small risk of infection or injury to surrounding structures.