Skin biopsy punch procedures are widely used, yet outcomes depend on the consistency with which the technique is performed. Even small variations in depth, site selection, or specimen handling can lead to non-diagnostic samples or repeat biopsies.
As demand for dermatologic and minor surgical procedures increases, this becomes more significant. The biopsy punch market is projected to reach approximately USD 4.853 billion by 2035, reflecting broader adoption across clinical settings.
With this expansion, consistency across cases is critical. The effectiveness of a skin biopsy punch depends less on the instrument itself and more on how precisely each step is performed.
In this blog, you’ll explore how the skin biopsy punch is used in clinical practice, including technique, size selection, and key factors that influence diagnostic accuracy and closure outcomes.
Key Takeaways:
- Skin biopsy punch is used for full-thickness sampling when tissue depth and architecture are required for accurate diagnosis.
- Diagnostic accuracy depends heavily on technique, including site selection, depth control, and specimen handling.
- A 4 mm punch is the most commonly used size, balancing adequate tissue sampling with manageable wound closure.
- Punch biopsy is preferred for inflammatory dermatoses, non-melanoma skin cancers, and clinically uncertain lesions.
- Technical errors such as superficial sampling, poor handling, or incorrect site selection can result in non-diagnostic results and necessitate repeat procedures.
What Is a Skin Biopsy Punch & How Does It Work?
In surgical practice, a skin biopsy punch is used to obtain a full-thickness tissue sample while maintaining control over specimen quality and closure.
It allows targeted sampling without committing to excision, particularly when depth and tissue architecture are required for diagnosis.
A skin biopsy punch is a cylindrical cutting tool, typically 2-8 mm in diameter, designed to remove a vertical core that includes all skin layers. Its effectiveness depends on controlled technique rather than force.
Here’s how the skin biopsy punch works in practice:

A skin biopsy punch functions as a precision sampling tool, where technique at each step influences specimen adequacy and downstream wound closure.
Understanding how a skin biopsy punch works also helps clarify the clinical situations in which it is most appropriately used.
When to Use a Skin Biopsy Punch in Clinical Practice?
In surgical practice, a skin biopsy punch is used when a full-thickness specimen is required without proceeding directly to excision. The decision depends on lesion characteristics, diagnostic requirements, and whether tissue depth will influence management.
Here’s when you should use a biopsy punch in clinical practice:
1. Inflammatory and Chronic Dermatoses
Most inflammatory conditions extend into the dermis, making superficial techniques unreliable for diagnosis. A skin biopsy punch is used to capture this depth while preserving tissue architecture, allowing evaluation of patterns across the epidermis and dermis together.
This reduces the risk of non-diagnostic superficial sampling and repeat procedures.
2. Suspected Non-Melanoma Skin Cancers
For lesions suspicious for basal cell carcinoma (BCC) or squamous cell carcinoma (SCC), assessing dermal involvement is often necessary before treatment.
A skin biopsy punch provides adequate depth to evaluate invasion and allows sampling of the most atypical portion of the lesion without committing to excision.
3. Lesions Where Tissue Architecture Matters
Certain diagnoses depend on the relationships among skin layers rather than on surface appearance alone. In these cases, a vertical specimen is required.
A skin biopsy punch preserves continuity among the epidermis, dermis, and subcutaneous tissue, thereby supporting accurate histopathological interpretation.
4. Clinically Uncertain Lesions
When the diagnosis is unclear, the goal is to sample the most representative area without over-treating the lesion.
A skin biopsy punch allows targeted sampling of heterogeneous lesions and provides tissue for histopathological evaluation to guide further management.
5. High-Throughput Clinical Settings
In routine clinical settings, a skin biopsy punch provides a predictable and time-controlled approach under local anesthesia.
It requires minimal instrumentation and produces a defect that can usually be closed with simple techniques, making it suitable for consistent, repeatable use.
In these settings, especially where multiple procedures are performed, bioabsorbable subcutaneous closure options such as SubQ It! 10 can help simplify post-procedure management by eliminating the need for staple removal.
Understanding when to use a skin biopsy punch in clinical practice also provides a clear foundation for following the step-by-step approach to the procedure.
7 Steps to Approach Skin Biopsy Punch Procedure
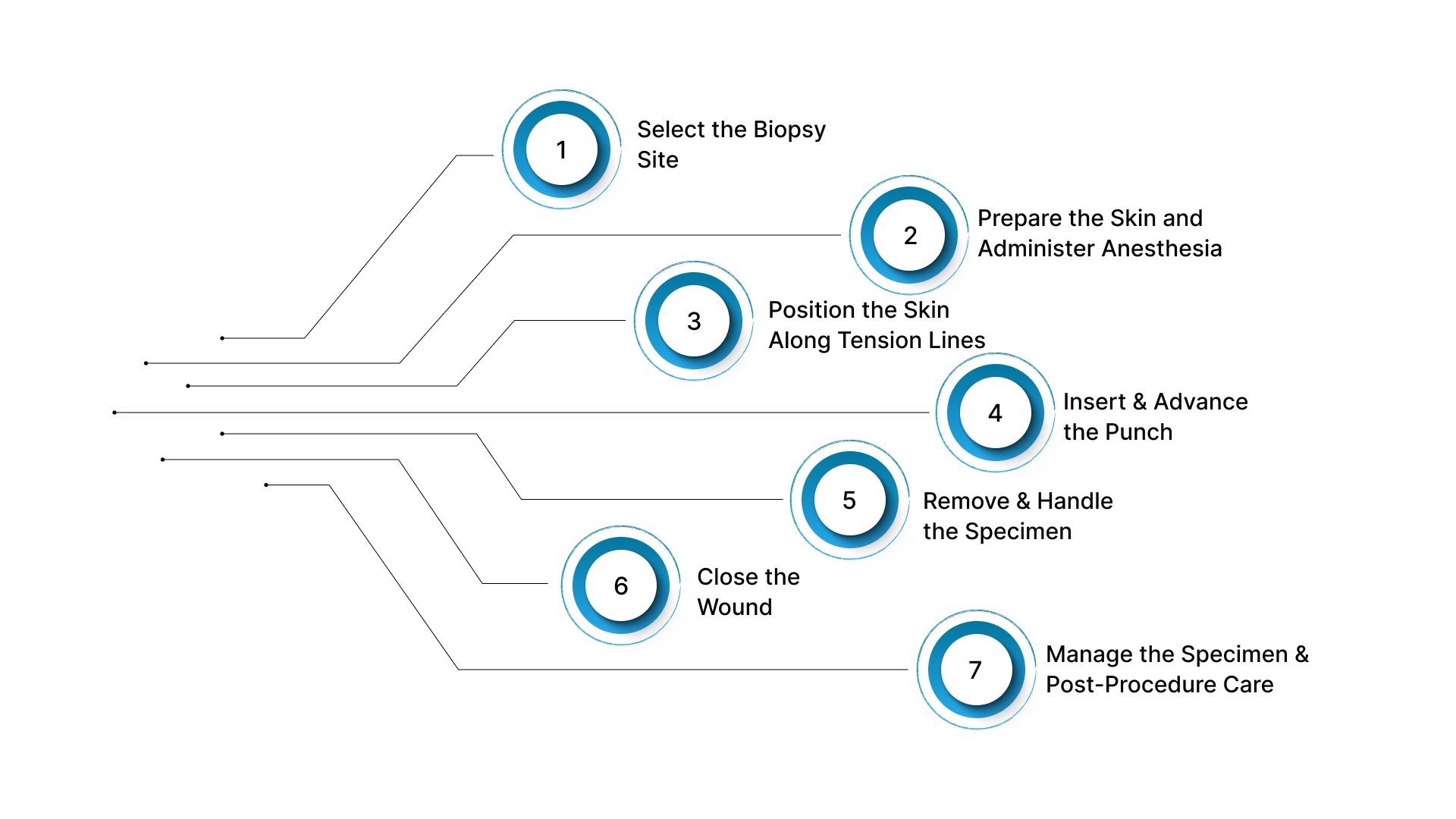
A skin biopsy punch procedure follows a defined sequence, where control over site selection, depth, and handling determines specimen adequacy and closure quality.
The objective is to obtain a representative, full-thickness sample while maintaining a predictable wound. Below are the seven steps to approach the skin biopsy punch procedure.
1. Select the Biopsy Site
Site selection determines whether the specimen will be diagnostic. The focus is on identifying the most representative portion of the lesion based on clinical presentation.
- Sample the active edge: In inflammatory lesions, the advancing margin better reflects ongoing pathology than the center.
- Target the most atypical area: In suspected malignancy, raised or irregular regions are more likely to capture diagnostic features.
- Avoid non-viable tissue: Necrotic or ulcerated areas may not represent underlying disease unless specifically indicated.
2. Prepare the Skin and Administer Anesthesia
Preparation should minimize tissue distortion while ensuring adequate anesthesia. A controlled approach improves both sampling accuracy and procedural flow.
- Clean the site properly: Chlorhexidine or povidone-iodine is used to reduce the risk of contamination.
- Use controlled local infiltration: Lidocaine is infiltrated locally to avoid excessive volume that may distort tissue.
- Allow full anesthetic effect: Waiting for the onset improves procedural control and reduces patient movement.
3. Position the Skin Along Tension Lines
Skin positioning affects both specimen shape and closure. Proper tension improves control during insertion and supports better wound approximation.
- Stretch perpendicular to tension lines: This stabilizes the tissue during punch insertion.
- Maintain uniform tension: Consistent tension helps produce a controlled specimen.
- Create an elliptical defect: Proper positioning supports easier closure with less tension.
4. Insert and Advance the Punch
Insertion is guided by technique rather than force. Depth is determined by tactile feedback during advancement.
- Use rotational motion: A steady twisting movement allows controlled advancement through tissue layers.
- Advance to subcutaneous tissue: Reaching superficial fat helps achieve full-thickness sampling.
- Recognize depth transition: A subtle loss of resistance typically indicates entry into subcutaneous tissue.
5. Remove and Handle the Specimen
Specimen handling directly affects histopathological interpretation. The goal is to extract the tissue without introducing distortion.
- Lift the specimen gently: A needle or skin hook allows controlled elevation without compression.
- Avoid the use of forceps: Forceps can introduce crush artifacts and distort tissue architecture.
- Release the base cleanly: Cutting with scissors preserves specimen integrity for evaluation.
6. Close the Wound
Closure depends on punch size and anatomical location. Alignment and tension control remain the priority for optimal healing.
- Use simple sutures: Most defects are closed with 1–2 interrupted sutures.
- Align with tension lines: Proper orientation reduces scar widening.
- Consider no closure for small defects: Smaller punches may be left unsutured in select cases.
7. Manage the Specimen and Post-Procedure Care
Specimen handling and post-procedure care influence both diagnostic reliability and healing outcomes. Immediate processing and clear instructions are required.
- Preserve the specimen immediately: Place it in formalin with correct labeling.
- Provide clear wound care guidance: Instructions should support proper healing.
- Plan suture removal timing: Timing varies by anatomical location and healing rate.
Alongside the step-by-step procedure, it is also important to understand the different biopsy punch sizes used in clinical practice.
Different Skin Biopsy Punch Sizes in 2026
Skin biopsy punch sizes have remained largely standardized, but how they are used in practice continues to change. Most punch biopsies fall within a predictable range, with a few sizes used consistently across clinical settings.
Below are the different types of skin biopsy punch sizes.
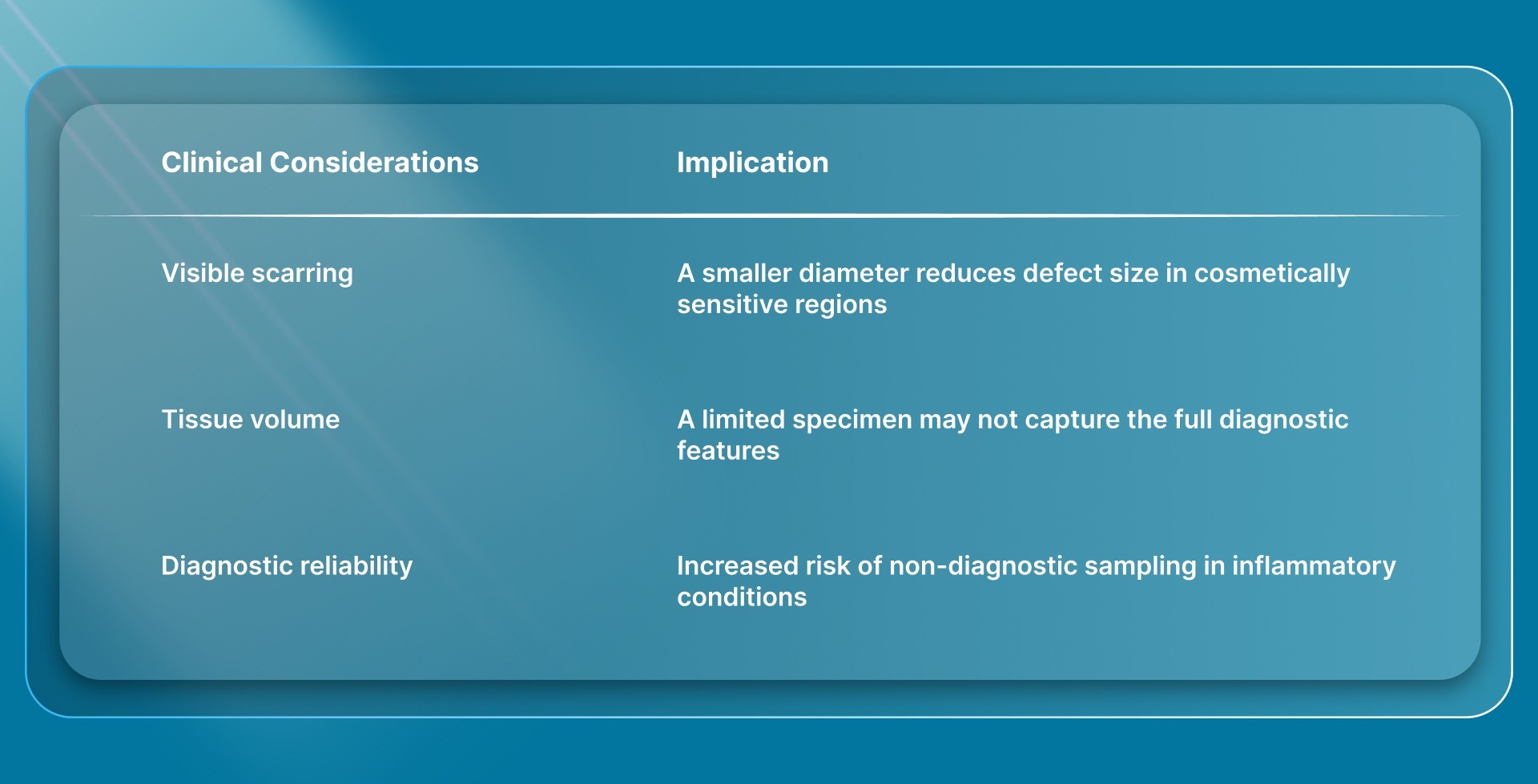
1. 2–3 mm Punches
Smaller punches are primarily used where defect size and cosmetic outcome are the main constraints. They are commonly used in facial areas or locations with limited skin laxity.
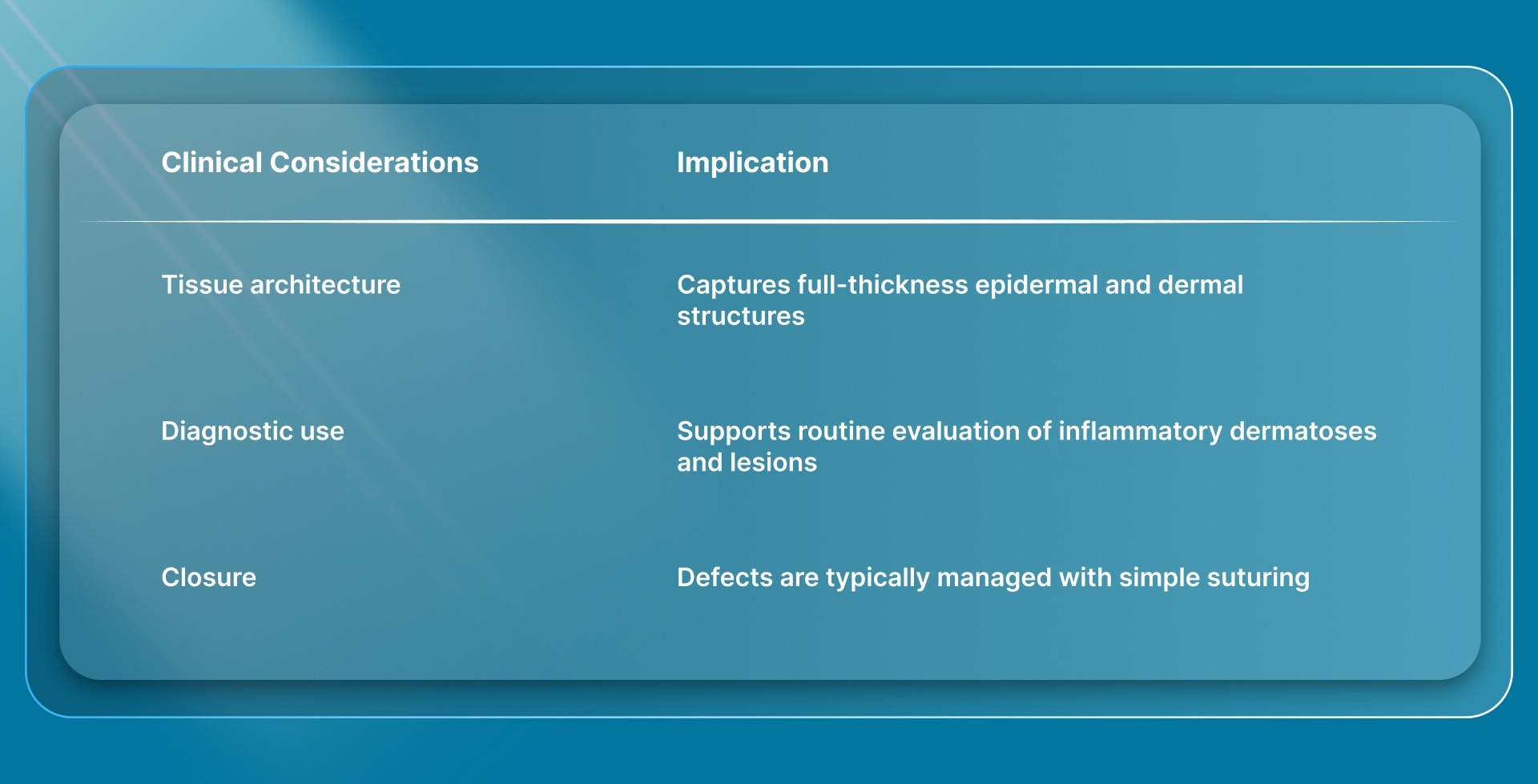
2. 4 mm Punch
The 4 mm punch remains the standard size for most diagnostic biopsies. It provides a balance between tissue adequacy and ease of closure.
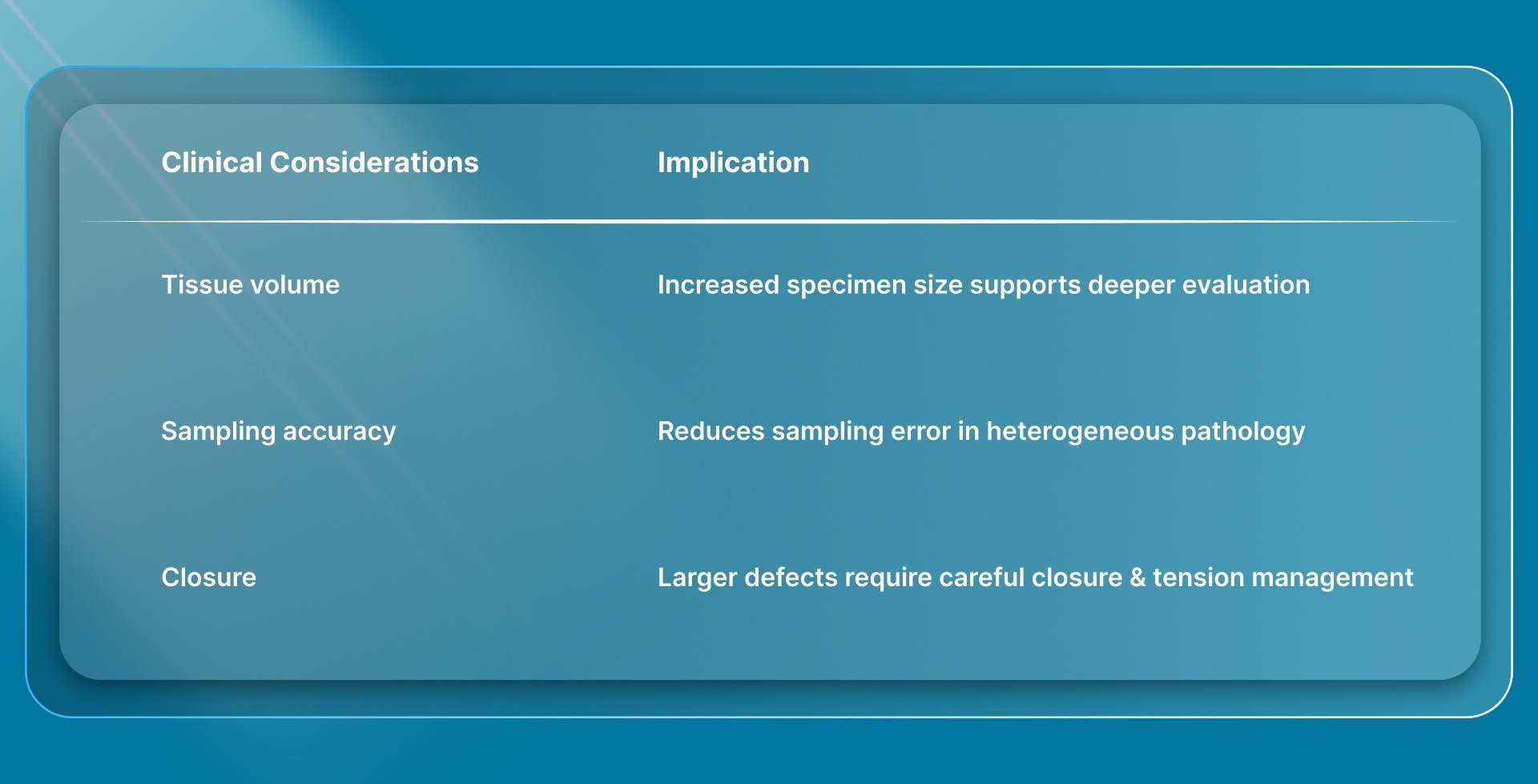
3. 5–6 mm Punches
Moderate-sized punches are used when additional tissue is required, particularly for deeper or more complex pathology.
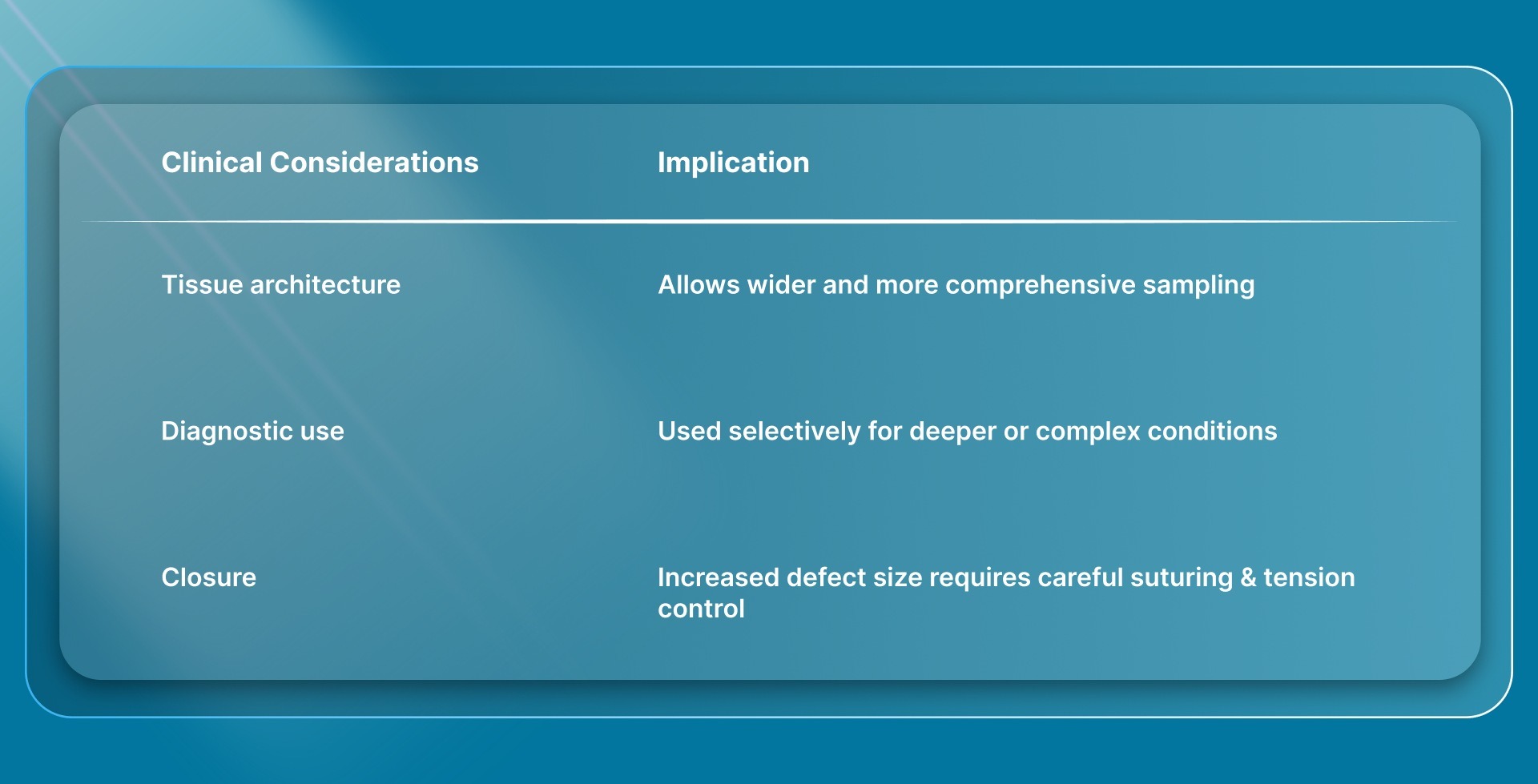
4. 7–8 mm Punches
Larger punches are used selectively when broader tissue architecture is required. Their use is less common in routine practice.
Beyond size selection, several technical factors also play a key role in determining the outcomes of skin biopsy punches in practice.
8 Technical Factors That Affect Skin Biopsy Punch Outcomes
Even when the correct technique is followed, outcomes from a skin biopsy punch can vary based on how consistently key technical variables are controlled.
These factors influence specimen quality, diagnostic reliability, and wound closure, often independent of the standard procedural sequence.
1. Specimen Representativeness
Outcome reliability depends on whether the sampled tissue reflects the underlying pathology. This is not only about where the biopsy is taken, but also how accurately the selected area represents disease activity.
- Sampling bias affects diagnostic accuracy: Non-representative areas can lead to discordance between clinical impression and pathology.
- Lesion heterogeneity increases variability: Mixed morphology requires precise targeting to avoid incomplete interpretation.
- Repeat biopsies may result from poor representativeness: Even technically correct procedures can fail if the sampled area is not appropriate.
2. Depth Consistency
Consistency in depth is critical to ensure that clinically relevant structures are included in the specimen. Variability at this stage can directly affect interpretation.
- Inconsistent depth leads to incomplete sampling: Failure to reach the dermis or superficial subcutaneous tissue can limit diagnostic value.
- Excessive depth generally does not improve diagnostic yield: in most cases, deeper penetration increases tissue disruption without adding useful information.
- Tactile feedback varies across sites and operators: Differences in resistance can affect depth control during insertion.
3. Edge Integrity of the Specimen
The condition of specimen edges influences how clearly tissue architecture can be interpreted. Mechanical distortion at this stage can reduce diagnostic clarity.
- Irregular edges can affect histological interpretation: Distortion may obscure structural relationships within the tissue.
- Excessive rotational force may affect tissue margins: Controlled advancement helps preserve specimen integrity.
- Uniform cylindrical specimens improve readability: Consistent shape supports more reliable evaluation.
4. Tissue Compression Effects
Mechanical pressure applied during extraction or handling can alter tissue structure. This effect is often subtle but clinically relevant.
- Compression can mimic or obscure pathology: Distorted cells may complicate interpretation.
- Handling technique influences artifact formation: Even brief pressure can affect specimen quality.
- Minimizing mechanical stress preserves architecture: Gentle handling reduces diagnostic interference.
5. Field Visibility During Sampling
Visibility at the time of sampling affects precision and control. Reduced clarity can introduce small but meaningful technical errors.
- Limited visibility affects placement accuracy: This can result in a suboptimal sampling location.
- Bleeding can obscure depth perception: It may make it harder to judge penetration and orientation.
- Maintaining a clear field supports consistent technique: Improved visibility enhances procedural control.
6. Defect Geometry and Tension Distribution
The shape and tension profile of the biopsy defect influence both closure and healing. These are affected by how the punch is applied, not just where it is placed.
- Irregular defect geometry increases closure difficulty: Non-uniform defects require additional adjustment.
- Uneven tension affects wound edge alignment: This may influence healing quality.
- Controlled technique supports predictable defect shape: Consistent execution improves closure efficiency.
7. Operator Variability
Differences in technique between operators can lead to variation in outcomes, even when using the same tools and approach.
- Technique variation affects reproducibility: Small differences in execution can influence results.
- Experience improves consistency: Familiarity with tissue response supports better control.
- Standardization reduces variability: A consistent approach improves reliability across cases.
8. Integration with Closure Strategy
Biopsy execution and closure should be considered together, as decisions made during sampling influence closure options and outcomes.
- Larger or irregular defects increase closure complexity: This may require more planning at the time of biopsy.
- Tension at closure is influenced by the initial technique: Poor execution can limit closure options.
- Planning closure during biopsy improves outcomes: Integrating both steps supports predictable healing.
Final Thoughts
Skin biopsy punch procedures do not end with tissue sampling. They extend to diagnostic reliability, wound-closure quality, and the overall healing experience that follows.
As expectations around consistency, cosmetic outcomes, and follow-up efficiency continue to change, the role of closure becomes more closely tied to procedural performance.
In this context, SubQ It! 10 offers a bioabsorbable subcutaneous closure system for incisions up to 10 cm in length.
Because the fasteners are absorbed over time, there is no need for a follow-up visit for removal, helping reduce post-procedure burden while supporting cleaner healing outcomes.
Contact us to explore how SubQ It! 10 fits into your workflow and supports post-biopsy closure.
FAQs
1. What can a skin punch biopsy detect?
Punch biopsy detects skin cancers (melanoma, basal cell, squamous cell), inflammatory conditions (psoriasis, eczema, lupus), infections, and precancerous lesions through microscopic examination.
2. Are skin punch biopsies painful?
Local anesthesia makes the procedure virtually painless. Patients feel only the initial needle stick, with mild soreness possible during healing.
3. How does anatomical location affect healing after a punch biopsy?
Areas with better blood supply, such as the face, heal faster, whereas the lower extremities may heal more slowly and have a higher risk of complications.
4. What is the difference between a punch biopsy and other biopsy techniques?
Punch biopsy provides a full-thickness cylindrical sample. Shave biopsy removes superficial layers, excisional biopsy removes the entire lesion, and incisional biopsy takes a wedge-shaped sample.
5. How should anticoagulated patients be managed during a punch biopsy?
Most minor skin procedures can be performed without stopping anticoagulants, but the bleeding risk should be assessed and managed with local measures.
6. Does a punch biopsy always provide a definitive diagnosis?
Not always. Diagnostic accuracy depends on site selection, depth, and lesion type, and some cases may require repeat or alternative biopsy methods.