The choice of skin closure method may prioritize efficiency, but it also influences factors beyond closure time. It affects postoperative care and the smoothness with which cases progress through the operating schedule.
With demand rising for faster, more consistent methods, the global surgical stapling devices market is projected to reach USD 9.89 billion by 2030, reflecting the operational weight of these decisions.
Skin clips are commonly used for their speed and consistency in linear incisions. However, their external placement and need for removal add steps beyond the procedure.
In this blog, you’ll explore how wound closure skin clips are evaluated in 2026 based on efficiency, follow-up burden, cosmetic outcomes, and workflow impact.
Key Takeaways:
- Skin clips provide fast, consistent closure of linear incisions but require removal and leave visible entry points on the skin.
- Sutures offer the highest control over tissue approximation and tension, making them suitable for complex or irregular wounds, though they increase closure time.
- Closure choice affects not just technique but also operating room time, follow-up workload, and overall case scheduling efficiency.
- Methods that require removal add an extra post-operative step, impacting clinic capacity and patient coordination
- Selecting the right closure depends on incision type, tissue tension, procedural context, and how the method fits into the full workflow
What Are Wound Closure Skin Clips?
Skin clips for wound closure are metal surgical staples placed through the skin to quickly approximate wound edges at the end of a procedure. In practice, surgeons use this method when closure speed and consistency are priorities, particularly for linear incisions.
Below are the key features of skin clips wound closure.
To place skin clips in context, it helps to compare them with other commonly used closure methods such as sutures and surgical staples.
How Skin Clips Compare With Sutures and Surgical Staples?
Surgeons evaluate closure methods based on closure time, control over tissue approximation, and post-operative management requirements.
Skin clips, sutures, and surgical staples each address these factors differently, which directly affects workflow and outcomes across procedures. Here’s how skin clips compare with sutures and surgical staples:
- Closure speed: Clips and staples close faster than sutures, reducing time in the operating room
- Tissue control: Sutures allow precise tension and edge alignment, suited for complex or irregular wounds
- Consistency of application: Clips and staples deliver uniform closure, while suturing depends on operator technique
- Follow-up requirements: Clips and staples need removal within 7–14 days, requiring an additional visit
- Cosmetic outcomes: Subcuticular sutures support better cosmetic results, while clips and staples may leave marks
- Workflow impact: Clips and staples improve case turnover, while sutures take longer but offer control
Skin clips, sutures, and staples each address specific closure needs, but they also introduce trade-offs between speed, control, and follow-up requirements.
For smaller incisions, bioabsorbable subcutaneous systems such as SubQ It! SU-10 is designed to support consistent closure beneath the skin, reduce closure time, and eliminate the need for a removal visit.
These comparisons also clarify the clinical situations where skin clips are most effective and where their limitations become evident.
When Are Skin Clips Used for Wound Closure & When Do They Fall Short?
Skin clips are used when rapid, straightforward closure of linear incisions is the priority. In practice, surgeons apply them selectively based on procedure type, anatomical location, and post-operative management considerations.
Here’s when skin clips wound closure is used:
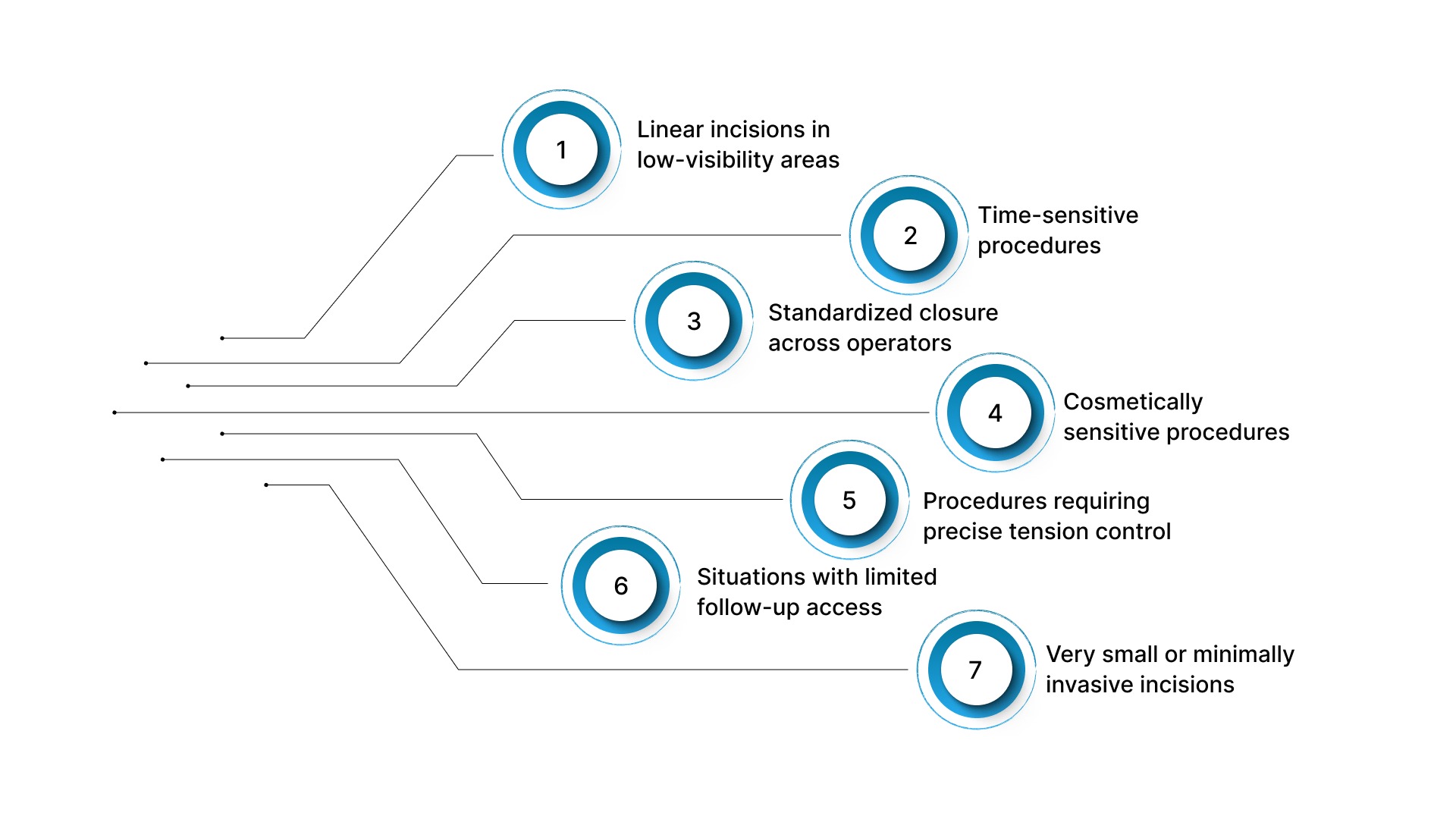
- Linear incisions in low-visibility areas: Commonly used for scalp, trunk, and certain orthopedic incisions where speed is important and cosmetic sensitivity is lower
- Time-sensitive procedures: Preferred in trauma or high-volume operating lists where reducing skin closure time supports overall OR (Operating Room) efficiency
- Standardized closure across operators: Requires less technical precision than suturing, enabling consistent application along linear incisions
These advantages also define where skin clips are less suitable.
Here’s when skin clips wound closure falls short of:
- Cosmetically sensitive procedures: External placement creates puncture points along the incision, which can affect scar appearance in visible areas
- Procedures requiring precise tension control: Clips do not allow fine adjustment across the wound, limiting their use in irregular or high-tension closures
- Situations with limited follow-up access: The need for post-operative removal introduces dependency on a return visit
- Very small or minimally invasive incisions: Less commonly used for small laparoscopic port sites where precise, low-profile closure methods are preferred
Understanding where skin clips perform well and where they have limitations also provides context for considering alternative closure options, including bioabsorbable subcuticular fasteners.
What Surgeons Need to Know About Bioabsorbable Subcuticular Fasteners?
Bioabsorbable subcuticular fasteners are used to approximate wound edges beneath the skin surface, rather than through it. For surgeons, this changes skin-level closure by removing external penetration while maintaining consistent edge approximation.
Below are the points outlining how these systems function in practice and where they impact the workflow.
1. Subcutaneous Placement
These fasteners are deployed within the dermal layer, holding tissue from beneath rather than crossing the skin surface. This changes how closure forces are applied across the incision.
- Internal tissue engagement: Fasteners anchor within the dermis rather than penetrating outward through the skin
- Subsurface tension distribution: Closure forces are applied beneath the surface, supporting even approximation along the incision
- No external puncture points: Avoids surface entry and exit marks along the skin
2. Bioabsorbable Material
The fasteners are made from medical-grade bioabsorbable polymers that gradually degrade during the healing period. This removes the need for a device-related removal step.
- Gradual absorption: Material breaks down over time as healing progresses
- No removal required: Eliminates the need for post-operative staple or suture removal
- Reduced follow-up dependency: Simplifies post-operative planning when closure does not require a return visit
3. Standardized Deployment
These systems are delivered through a single-use applicator, enabling repeatable placement along the incision.
- Controlled deployment: Each fastener is placed using a consistent mechanical action
- Reduced technique dependency: Less reliance on manual suturing precision for skin-level closure
- Uniform spacing: Supports consistent closure across linear incisions
4. Time Efficiency in Closure
These systems are designed to reduce skin closure time, particularly when compared to manual subcuticular suturing.
- Faster than manual suturing: Decreases time required for skin closure
- Scales with incision length: Time savings become more relevant in longer or multiple incisions
- Supports OR efficiency: Helps maintain procedural timelines in high-volume settings
5. No Scheduled Removal Workflow
Because the fasteners are absorbed, closure does not require a dedicated removal visit, which changes post-operative workflow.
- No removal appointment: Eliminates an additional clinical step tied to the closure method
- Lower clinic workload: Reduces time spent on routine removal visits
- Improved patient convenience: Particularly relevant where follow-up access is limited
6. Cosmetic Alignment With Subcuticular Techniques
The absence of external penetration aligns these systems with subcuticular closure approaches from a cosmetic standpoint.
- No surface puncture marks: Avoids patterns associated with externally placed closure methods
- Supports clean incision lines: Maintains a uniform appearance along the wound
- Comparable cosmetic outcomes: Consistent with results expected from subcuticular suturing techniques
A closer look at bioabsorbable subcuticular fasteners also provides the context needed to compare them directly with skin clips in surgical practice.
Skin Clips vs Bioabsorbable Fasteners for Wound Closure
When deciding between skin clips and bioabsorbable subcuticular fasteners, surgeons typically weigh the speed of external closure against the under-the-skin closure workflow.
The difference is not just in how the incision is closed, but also in how the case ends and what follows.

Beyond material and technique differences, practical factors such as operating room time, follow-up requirements, and overall case throughput also influence the choice of closure method.
How OR Time, Follow-Up Visits, and Case Throughput Affect the Choice of Closure?
Closure selection influences more than technique. It affects total procedure time, postoperative workload, and the efficiency with which cases can be scheduled and completed within a given operating day.
Below are the points that focus on how these factors impact real-world workflow.
1. OR Time and Closure Efficiency
Skin closure is the final step of a procedure, and the time required varies by the method used. Differences at this stage directly contribute to the overall case duration.
- Closure time contributes to total case length: Manual suturing typically takes longer than device-based methods, particularly in longer incisions
- Effect across multiple cases: In multi-case schedules, small time differences per case can influence overall workflow timing
- Impact on OR utilization: Shorter closure times help maintain procedural flow and reduce delays between cases
2. Follow-Up Visits and Post-Operative Workflow
Some closure methods require a separate postoperative step for removal, extending care beyond the procedure itself. This affects both clinic operations and patient coordination.
- Removal-related appointments: Certain closure methods require a scheduled visit specifically for device removal
- Clinic scheduling impact: These visits occupy time that could otherwise be used for consultations or follow-up care
- Dependence on patient compliance: Timely removal depends on patient availability and adherence to follow-up schedules
3. Case Throughput and Practice Capacity
When closure time and post-operative requirements are considered together, they influence how many procedures can be completed within a defined schedule.
- Cumulative effect of time per case: Differences in closure time can affect how many cases fit into a single operating session
- Post-operative workload considerations: Methods that eliminate removal steps reduce additional clinic activity
- Scheduling consistency: Fewer required follow-up steps simplify coordination across operating and clinic schedules
These operational considerations ultimately inform broader decision-making, shaping the selection of the right wound-closure method in 2026.
How to Choose the Right Wound Closure Method in 2026?
Selecting a wound closure method is a case-specific decision based on incision characteristics, tissue behavior, procedural requirements, and post-operative considerations.
The objective is to choose an approach that supports reliable edge approximation, procedural efficiency, and manageable follow-up, without introducing unnecessary variability.
Here’s how you can choose the right wound closure method:
1. Incision Profile and Geometry
The shape, length, and depth of the incision influence how easily wound edges can be approximated and how much control is required during closure.
- Linear incisions: Can be managed with methods that provide consistent approximation along the incision
- Irregular or complex wounds: Require techniques that allow precise adjustment of edge alignment
- Incision length considerations: Closure method should scale with length without increasing variability or closure time disproportionately
2. Tissue Characteristics and Tension
Tissue behavior varies by anatomical location, making tension management a key factor in selecting a closure.
- Low-tension areas: Allow a broader range of closure options with predictable outcomes
- Variable tension zones: Require methods that maintain consistent approximation across the incision
- High-stress regions: Benefit from approaches that distribute closure forces effectively to maintain wound integrity
3. Procedural Context
The type of procedure and how closure fits within it influence method selection.
- Minimally invasive procedures: Require controlled closure suited to smaller incisions
- Open procedures: Need methods that can handle longer incisions efficiently
- Multiple incisions: Increase the importance of consistency and efficiency across repeated closures
4. Post-Operative Management Requirements
Closure methods differ in their effects on postoperative care and follow-up.
- Removal requirements: Some methods require a dedicated follow-up step, while others do not
- Follow-up reliability: Closure choice may depend on how predictable patient return visits are
- Care pathway simplicity: Methods that reduce post-operative steps can streamline overall management
5. Consistency and Reproducibility
Consistency becomes more relevant in settings where predictable outcomes are required across multiple cases.
- Technique-dependent methods: Require higher manual precision and may vary with operator experience
- Standardized methods: Enable repeatable placement with reduced variability
- Scalability: Consistency becomes increasingly important as case volume increases
Final Thoughts
Closure decisions affect more than how an incision is closed. They influence procedural flow, consistency across cases, and the amount of post-operative follow-up required.
In this context, SubQ It! SU-10 offers a bioabsorbable subcutaneous closure system designed for small and laparoscopic incisions, supporting closures up to 10 cm while reducing closure time by approximately 5 minutes per case.
Because the fasteners are placed beneath the skin and are bioabsorbable, there is no need for a follow-up visit to remove them.
Contact us to explore how SubQ It! SU-10 can support small-incision closure efficiency and post-operative workflow in your practice.
FAQs
1. Are skin clips suitable for patients prone to hypertrophic or raised scarring?
Skin clips may be considered more carefully when scar appearance is a priority, as external skin penetration can leave visible marks along the incision. In such cases, closure methods that avoid surface puncture may be evaluated.
2. Do skin clips affect post-operative wound care or showering timelines?
Wound care protocols depend primarily on the procedure, incision location, and clinical guidance rather than the closure device alone. However, externally placed clips require routine monitoring for local irritation, drainage, or loosening.
3. Can skin clips be used alongside deep dermal or fascial sutures?
Yes. In layered closure, deeper tissues are typically approximated with sutures before skin clips are applied. This approach maintains structural support while allowing faster skin-level closure.
4. Are skin clips practical when post-operative follow-up is uncertain?
This can be a limitation. Because skin clips require removal, their use depends on reliable post-operative access. In cases where follow-up timing is uncertain, alternative methods may be considered.
5. How should closure be approached in revision or re-entry procedures?
Closure selection in revision cases depends on tissue quality, prior scarring, and incisional tension. When more precise control over tissue handling is required, methods that allow adjustment along the wound may be preferred.
6. What factors matter most when selecting a closure method in outpatient procedures?
Key considerations include incision length, tissue tension, cosmetic visibility, and the reliability of follow-up. In outpatient settings, removal requirements can influence workflow just as much as closure time.