Skin closure is often treated as a routine final step, yet it is one of the most visible determinants of surgical outcomes. Poor technique can lead to unnecessary scarring, uneven wound edges, and patient dissatisfaction, even when the procedure itself is technically sound.
Traditional surface closure methods can leave visible marks or create tension across the incision, particularly in cosmetically sensitive areas. Subcuticular skin closure addresses this by placing sutures within the dermis, allowing precise edge approximation without external stitch marks while supporting consistent healing.
The advantage is clear, but so is the challenge. This technique demands greater precision and time, making outcomes highly dependent on surgical skill.
This blog explores when subcuticular closure is the right choice and how to use it effectively in modern surgical practice.
TL;DR
- Intradermal closure technique that achieves wound approximation without epidermal penetration, reducing surface disruption and visible suture marks.
- Best suited for clean, low-tension incisions, where controlled dermal alignment is required over rapid closure.
- No significant difference in surgical site infection rates compared with staples, adhesives, or other closure methods.
- Compared with staples, it is generally associated with fewer wound complications and improved cosmetic outcomes, though closure time is longer.
- Outcomes depend primarily on proper tension control, technique precision, and appropriate case selection, rather than the closure method alone.
What Is Subcuticular Skin Closure?
Subcuticular skin closure is a suturing technique in which stitches are placed within the dermis, just beneath the epidermis, rather than passing through the outer skin surface. In practical terms, the wound is closed intradermally, so most of the suture material remains hidden under the skin.
This approach is primarily used when the goal is precise wound edge approximation with minimal visible scarring, particularly in clean, low-tension surgical incisions.
What Is the Standard Technique for Subcuticular Skin Closure?
Rather than a rigid checklist, the technique is best understood as a controlled sequence focused on dermal alignment and tension distribution.
Here’s how it works in clinical practice:
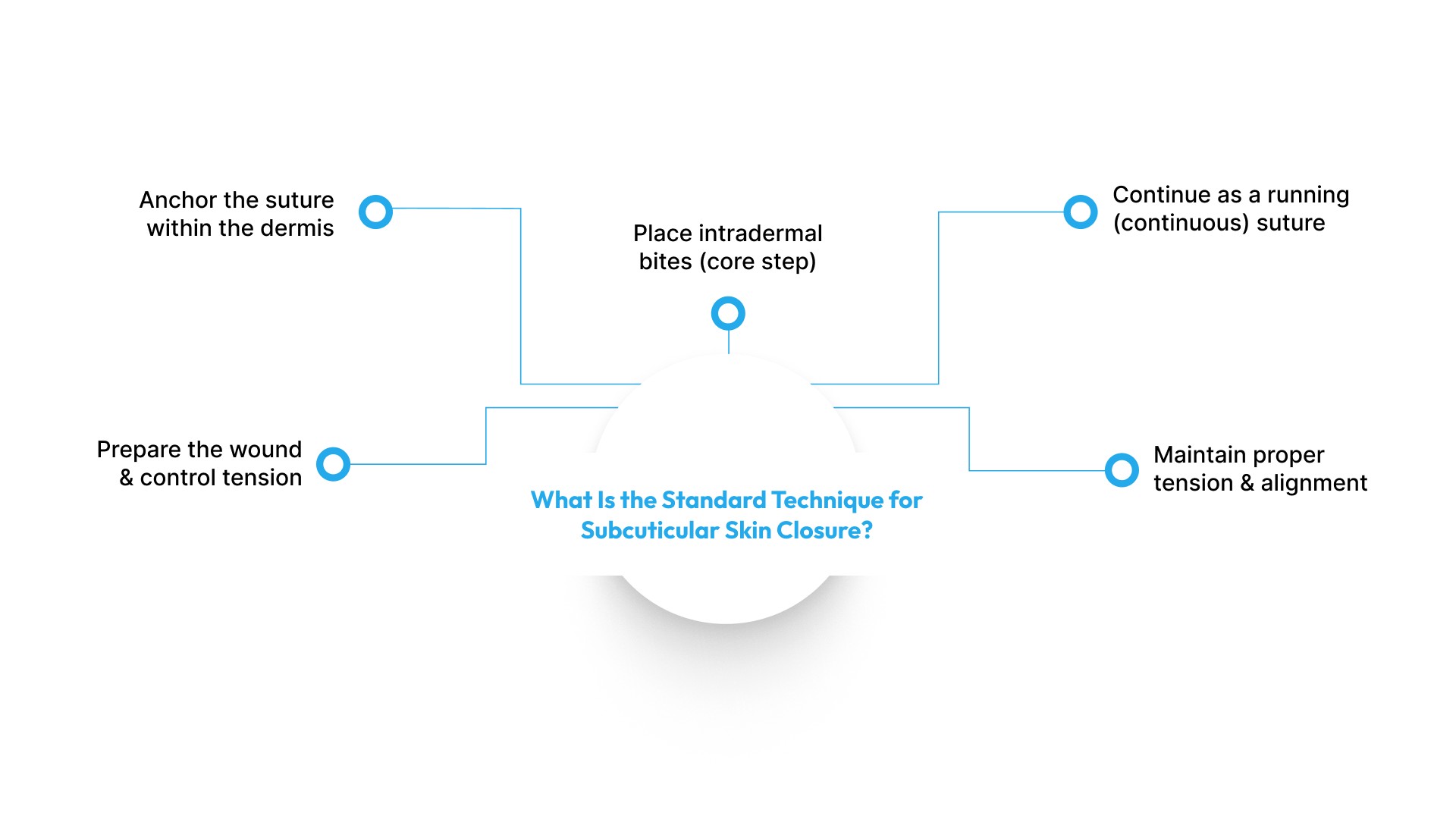
1. Prepare the wound and control tension
- Ensure the wound is clean, hemostatic, and well approximated
- Place deep dermal sutures where required
Note: Subcuticular sutures are not designed to bear significant tension independently; they function as a superficial closure layer
2. Anchor the suture within the dermis
- Closure begins at one end of the incision
- A buried intradermal knot or anchoring pass is used
- Typically performed with absorbable monofilament sutures (e.g., PDS, Monocryl)
3. Place intradermal bites (core step)
- The needle travels horizontally within the dermis
- Each bite is placed:
- Parallel to the incision
- Alternating between wound edges
- Depth and spacing are kept consistent
This reduces:
- epidermal punctures
- suture-track scarring
- surface irritation
4. Continue as a running (continuous) suture
- The suture is advanced along the incision in a continuous pattern
- Modern best practice:
- Small bites (≈4–5 mm apart)
- Close to wound edge (≈5–8 mm)
5. Maintain proper tension and alignment
- The goal is edge approximation, not compression
- Excess tension can impair perfusion
A well-executed closure results in:
- Flat, well-aligned edges
- No inversion or bunching
What Types of Sutures Are Used in Subcuticular Skin Closure?
The choice of suture material in subcuticular closure is not arbitrary; it directly affects wound healing, infection risk, and cosmetic outcome. In practice, sutures are broadly classified based on absorbability and filament structure, with clear preferences supported by current literature.
1. Absorbable Sutures (Preferred in Most Cases)
Absorbable sutures are the standard choice for subcuticular closure, particularly when a fully buried technique is used.
- Designed to gradually lose tensile strength and degrade in vivo
- Can be completely buried within the dermis, avoiding the need for removal
- Reduce external exposure → lower contamination risk
Common materials:
- Poliglecaprone (Monocryl)
- Polydioxanone (PDS)
- Polyglactin (Vicryl)
From a clinical standpoint, slowly absorbable monofilament sutures are preferred because they provide the following:
- Sustained support during healing
- Lower tissue reactivity
- Better cosmetic outcomes
This shift toward synthetic absorbable materials has significantly expanded the use of subcuticular closure across surgical settings.
2. Non-Absorbable Sutures (Selective Use)
Non-absorbable sutures are less commonly used but remain relevant in specific scenarios.
- Do not degrade in tissue
- Typically require removal after healing
- In subcuticular techniques, the ends are often left external, increasing exposure risk
Common materials:
- Nylon (polyamide)
- Polypropylene (Prolene)
While they can offer consistent tensile strength, their use in subcuticular closure is limited because:
- Externalized ends may increase contamination risk
- They may reduce the advantage of a fully buried, cosmetic closure
Monofilament vs Multifilament Sutures (Why It Matters)
Beyond absorbability, sutures are also classified by structure:
Monofilament sutures
- Single-strand structure
- Lower infection risk due to reduced bacterial adherence
- Slightly more difficult handling
Multifilament (braided) sutures
- Multiple fibers twisted or braided
- Easier handling and knot security
- Higher potential for bacterial colonization
Recent evidence indicates that monofilament sutures are associated with a lower risk of surgical site infection compared to multifilament sutures in subcuticular closure.
4 Reasons Surgeons Prefer Subcuticular Skin Closure
Subcuticular skin closure offers a distinct set of advantages in appropriately selected wounds, particularly clean, low-tension surgical incisions. Its benefits are best understood across cosmetic outcomes, clinical performance, and patient experience, rather than as isolated features.
1. Improved cosmetic outcomes
Subcuticular sutures are placed within the dermis, avoiding external puncture marks.
- Results in smoother scars without crosshatch (“railroad track”) markings
- Supports more uniform edge approximation
- Particularly useful in cosmetically sensitive areas
From a clinical perspective, the technique is primarily chosen when scar quality is a priority outcome.
2. Favorable clinical outcomes (vs staples)
Evidence suggests that subcuticular closure provides a comparable safety profile with specific advantages over staples.
- No clear difference in surgical site infection (SSI) compared to other closure methods
- Reduced wound complications vs staple (moderate-certainty evidence)
- May lower risk of:
- Wound dehiscence
- Hypertrophic scarring
These benefits are most relevant in planned surgical incisions where healing quality is prioritized.
3. Higher patient satisfaction and comfort
Patient-reported outcomes consistently favor subcuticular techniques.
- Higher satisfaction scores vs transdermal sutures and staples
- Improved comfort due to:
- Absence of external sutures
- Reduced skin irritation
- No need for suture removal when absorbable materials are used
Importantly, satisfaction reflects a combination of cosmesis, comfort, and convenience, rather than cosmetic outcome alone.
4. Continuous tension distribution
The running intradermal pattern allows:
- Even distribution of tension along the incision
- Reduced localized stress points
- More consistent wound edge alignment
In practice, this contributes to stable healing, provided underlying tension has been adequately managed.
Subcuticular Skin Closure vs Other Methods: Key Clinical Differences
Subcuticular sutures are one of several established skin closure methods. Their role is best understood in comparison to alternatives—each technique offers trade-offs in speed, cosmetic outcome, and complication profile, depending on the clinical context.
| Parameter | Subcuticular Sutures | Skin Staples | Tissue Adhesives | Interrupted Sutures |
|---|---|---|---|---|
| Closure Time | Slower | Faster | Fastest | Moderate |
| Infection Risk | Comparable | Comparable | Comparable | Comparable |
| Complications | Lower vs staples | Higher risk | Comparable | Depends on wound |
| Cosmesis | Better | Less favorable | Good (selected cases) | More visible scarring |
| Tension Handling | Low–moderate | Moderate | Low | High |
| Use Case | Clean, low-tension wounds | Long incisions, speed priority | Small, superficial wounds | Irregular/high-tension wounds |
1. Subcuticular Sutures vs Skin Staples
This is the most studied comparison in surgical literature.
Key differences:
- Closure time: Staples are faster and reduce operative time
- Infection risk: No significant difference in surgical site infection (SSI) rates
- Wound complications: Subcuticular sutures are associated with fewer complications, including wound separation
- Cosmesis and satisfaction: Sutures generally provide better cosmetic outcomes and higher patient satisfaction
2. Subcuticular Sutures vs Tissue Adhesives (Skin Glue)
Tissue adhesives are increasingly used for low-tension, superficial wounds.
Key differences:
- Infection and complications: No clear difference compared to subcuticular sutures
- Application time: Adhesives are faster and easier to apply.
- Strength and control: Sutures provide greater structural support, especially in deeper or longer incisions
- Use case limitation: Adhesives are suitable only for small, low-tension wounds.
3. Subcuticular Sutures vs Transdermal (Interrupted) Sutures
Traditional interrupted sutures are still widely used, especially in variable or high-tension wounds.
Key differences:
- Technique: Subcuticular sutures run intradermally and continuously, while interrupted sutures pass through the full skin thickness
- Cosmetic outcome: Subcuticular closure reduces visible suture marks
- Tension handling: Interrupted sutures provide better control in high-tension or irregular wounds
- Flexibility: Interrupted sutures allow individual stitch adjustment or removal if needed
SubQ It!: Bioabsorbable Subcuticular Skin Closure Approach

Traditional metal staples enable rapid skin closure but are externally placed, require removal within 7–10 days, and can leave visible “railroad-track” scarring.
SubQ It! takes a different approach, using bioabsorbable subcuticular fasteners beneath the skin that resorb over time, eliminating removal and enabling a more refined closure result.
- Subcuticular bioabsorbable closure: Utilizes bioabsorbable fasteners placed beneath the skin to maintain wound approximation during healing, with the material gradually resorbing over time and eliminating the need for removal.
- No removal requirement: Avoids external removal procedures by relying on internal, absorbable fixation rather than external metal staples.
- Subcutaneous placement approach: Fasteners are positioned below the skin surface, preventing external exposure and providing internal support throughout the healing process.
- Applicability across incision lengths: Suitable for a range of incision sizes, from small laparoscopic port sites to longer surgical incisions, depending on the device configuration.
- Device variants:
- SubQ It! 10: intended for closures up to 10 cm, typically small or laparoscopic incisions
- SubQ It! 25: intended for closures up to 25 cm, used for longer surgical incisions
Final Thoughts
Subcuticular skin closure remains a reliable technique when wound approximation, cosmetic outcome, and controlled healing are priorities. Its primary strength lies in achieving precise dermal alignment while minimizing surface disruption, particularly in clean, low-tension surgical incisions.
Compared to external closure methods, its performance is defined less by speed and more by consistency in tissue approximation and long-term scar quality. When appropriately indicated, it offers a balanced profile of clinical stability and aesthetic benefit without increasing infection risk.
For cases where a shift toward internal, bioabsorbable closure is preferred, SubQ It! provides a subcuticular fastening system designed to support wound approximation beneath the skin with no requirement for removal. This approach helps maintain closure efficiency while reducing external exposure in suitable surgical applications.
To learn more about how SubQ It! can be integrated into your surgical workflow, connect with the SubQ It! team.
FAQs
1. What is subcuticular skin closure?
Subcuticular skin closure is a suturing technique where absorbable or non-absorbable sutures are placed within the dermis to approximate wound edges without penetrating the epidermis.
2. Is subcuticular closure better than staples?
Subcuticular sutures and staples show similar infection rates, but subcuticular closure is associated with better cosmetic outcomes and fewer wound complications in multiple studies.
3. Does subcuticular suturing reduce infection risk?
No consistent difference in surgical site infection rates has been demonstrated between subcuticular sutures and staples, adhesives, or other closure methods.
4. When is subcuticular closure used?
It is used in clean, low-tension surgical incisions where precise wound edge approximation and improved cosmetic outcomes are required.
5. What are the advantages of subcuticular sutures?
Advantages include improved scar appearance, absence of external suture marks, and higher patient satisfaction compared to transdermal sutures and staples.
6. Do subcuticular sutures need to be removed?
Absorbable subcuticular sutures do not require removal as they gradually degrade within the tissue over time.
7. Which is better for cosmetic outcomes: sutures or staples?
Subcuticular sutures generally provide better cosmetic outcomes than staples due to the absence of external puncture marks.