Reported surgical site infection (SSI) rates in gastrointestinal (GI) surgery fall anywhere from 1.0% to 25.6%, with colorectal cases at the upper end. That range makes the skin closure method an important consideration in GI procedures.
Subcuticular sutures consistently score higher on cosmetic outcomes and patient satisfaction than metal staples. Staples are faster to place, but they require removal and leave railroad-track scarring that patients notice.
This post covers the evidence on subcuticular sutures versus staples in GI surgery. It includes data on infection, scarring, closure time, and practical workflow considerations.
Key Takeaways
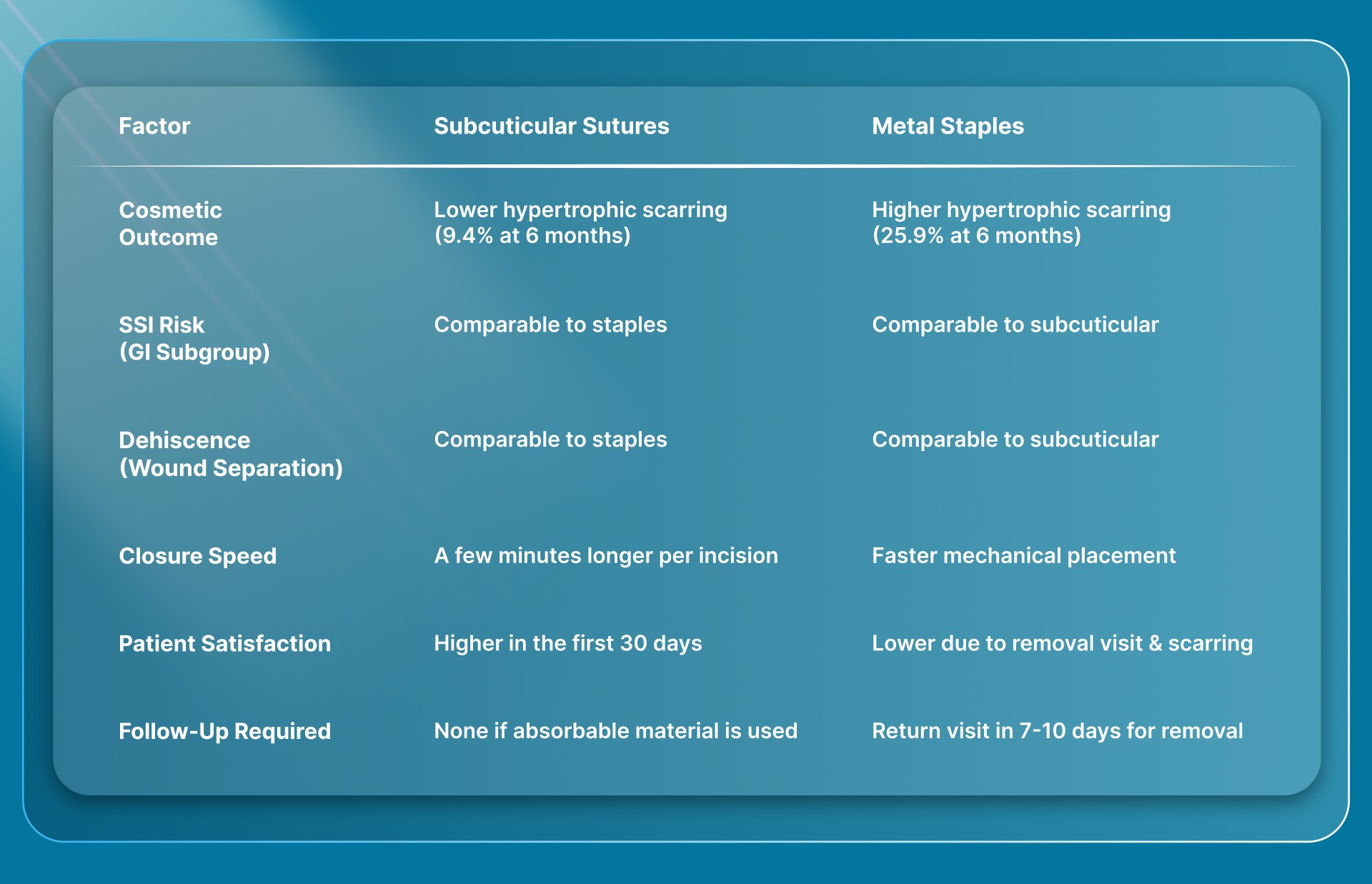
- Subcuticular sutures in GI surgery produce significantly less raised scarring compared to metal staples, with one study showing 9.4% versus 25.9% at six months.
- A pooled analysis of 7 randomized controlled trials (RCTs) found no meaningful difference in SSI rates between subcuticular sutures and staples in abdominal surgery overall.
- In the GI surgery subgroup specifically, subcuticular closure showed a similar infection risk to stapling, making other factors like cosmesis and convenience the deciding variables.
- Subcuticular continuous sutures received higher cosmetic ratings from both patients and clinicians compared to interrupted closure techniques.
- The main tradeoff with subcuticular suturing is closure speed, as it adds a few extra minutes per incision compared to stapling.
What Are Subcuticular Sutures in Gastrointestinal Surgery?
Subcuticular sutures are a skin closure technique where the suture runs horizontally through the layer just below the skin surface, never piercing the outer skin. In GI surgery, this technique closes abdominal incisions after procedures like colorectal resections, cholecystectomies, and hernia repairs.
The suture material sits entirely beneath the skin. That's why these closures don't leave the puncture marks you see with metal staples or interrupted stitches.
Here's a practical example. After a laparoscopic appendectomy, a surgeon using subcuticular closure would place a continuous running suture through the deeper skin layer of each port-site incision. The suture material, if absorbable, dissolves over weeks.
The patient never needs a follow-up visit for removal. The healed incision typically shows only a thin line rather than a row of dot-shaped marks on either side.
Compare that to metal staples, which sit on the skin surface and grip through both sides of the wound edge. Staples are fast to place but require a separate removal appointment after surgery.
The puncture sites from staple legs often produce what surgeons call railroad-track scarring. These are small paired marks running alongside the incision line.
Why Does Skin Closure Method Matter in GI Surgery?
Skin closure method matters in GI surgery because this specialty carries one of the highest infection risks across surgical disciplines. Reported SSI rates for GI procedures fall anywhere from 1.0% to 25.6%, with colorectal cases at the upper end.
Every decision that can reduce complications, including how you close the skin, deserves attention.
- Infection risk: GI procedures often involve contaminated or clean-contaminated surgical fields, making the skin closure method a factor in wound healing outcomes.
- Scar quality: Patients increasingly notice and care about abdominal scarring, even after procedures they'd consider medically necessary rather than cosmetic.
- Follow-up needs: Metal staples require a return visit for removal at 7 to 10 days, adding scheduling, staffing, and patient travel costs to every case.
- Financial impact: In colorectal surgery, an SSI can drive inpatient care costs up by 2 times and post-discharge expenses within 30 days up by 6 times.
Even when infection rates between closure methods are statistically similar, a single SSI in GI surgery carries high downstream costs. Surgeons comparing sutures versus staples for their own practice should weigh these financial and logistical realities alongside the clinical data.
How Do Subcuticular Sutures Compare to Metal Staples for GI Surgery Outcomes?
Subcuticular sutures consistently outperform metal staples on cosmetic outcomes while matching or slightly improving infection and wound separation rates in GI surgery. The tradeoff is closure speed.
Staples are faster to place, but the clinical advantages of subcuticular closure are measurable across studies. For surgeons weighing their options for skin closure, the comparison below covers the key outcome areas.
Each of these outcome areas carries practical weight beyond the numbers. Here's what the data looks like in context.
Scarring and Cosmetic Results
In a matched comparison of 85 liver resection patient pairs, raised scar formation at six months reached 9.4% in the subcuticular group versus 25.9% in the staple group. That's a statistically significant difference in a population undergoing major abdominal surgery.
A separate meta-analysis of 10 RCTs confirmed that subcuticular continuous sutures received higher cosmetic ratings from both patients and clinicians on visual analog scales. The cosmetic advantage held up consistently across the included studies.
For patients undergoing GI surgery, where abdominal scars are visible during everyday activities, this difference affects long-term satisfaction.
Surgical Site Infection Rates
A pooled analysis of seven RCTs with 3,705 patients showed no meaningful difference in SSI rates between subcuticular sutures and staples for skin closure across abdominal procedures. When the authors looked at the GI surgery subgroup alone, the infection risk remained similar between both methods.
A 2023 study of 346 patients having hepatobiliary and pancreatic procedures, reported SSI rates of 4.62% with subcuticular closure and 9.82% with staples. The result is worth noting for surgeons handling complex GI cases.
Closure Speed and OR Time
This is where staples have historically held the advantage. Subcuticular suturing adds a few extra minutes per incision compared to stapling. That difference adds up across a full day of surgery cases.
For surgeons who prioritize OR efficiency, this time penalty has been the main reason to stick with staples despite the cosmetic tradeoff.
Bioabsorbable subcuticular closure systems now address this speed difference directly. SubQ It! is a bioabsorbable skin closure system that places dissolving dermal fasteners beneath the skin at stapler speed. The fasteners never pierce the outer surface and absorb naturally after healing is complete.
The SubQ It! SU-25 variant closes incisions up to 25 cm and saves approximately 25 minutes per case compared to manual subcuticular suturing. For GI surgeons who've avoided subcuticular closure because of the time cost, that tradeoff no longer applies.
Which GI Procedures Benefit Most From Subcuticular Closure?
Subcuticular closure benefits GI procedures where infection risk, scar appearance, or follow-up convenience are priorities. The technique works across incision sizes, from small laparoscopic port sites to longer midline incisions.
The practical advantages vary by procedure type:
- Laparoscopic cholecystectomy: Trocar incisions are small and often placed in visible areas of the abdomen. Subcuticular closure avoids the paired puncture marks that staples leave on these compact incisions. Bioabsorbable wound closure options are especially practical here, since the incisions may be too small for standard stapler devices.
- Colorectal resection: These cases carry the highest SSI rates in GI surgery, and midline incisions are long enough that scar quality is noticeable. A study of patients undergoing complex abdominal surgery showed a trend toward lower SSI with subcuticular closure compared to staples.
- Laparoscopic appendectomy: Port-site incisions heal better cosmetically with the subcuticular technique, and the patient population often skews younger, making long-term scar appearance more important.
- Hernia surgery: Both open and laparoscopic approaches involve incisions where patients have clear sightlines to their scars during recovery, making cosmetic outcome a practical concern.
The clinical evidence doesn't limit subcuticular closure to any single procedure type. The choice depends on the surgeon's assessment of each patient's infection risk, incision length, and whether the time investment is justified by the expected cosmetic and clinical benefit.
What Should Surgeons Consider When Choosing Closure for GI Cases?
The right closure method depends on the specific clinical scenario, not on habit. Surgeons should weigh incision characteristics, patient factors, and practice logistics before defaulting to either staples or subcuticular sutures.
- Incision length: Short laparoscopic incisions are well-suited to subcuticular closure. Longer incisions historically favored staples for speed, but the SubQ It! SU-25 variant now handles incisions up to 25 cm with bioabsorbable dermal fasteners, removing that time tradeoff.
- Wound contamination class: Clean-contaminated and contaminated GI cases may benefit from keeping closure materials beneath the skin surface rather than placing external staples through potentially compromised tissue.
- Patient profile: Patients with obesity, diabetes, or other wound healing risk factors deserve extra consideration. The subcuticular technique avoids external puncture sites that could serve as entry points for infection.
- Practice setting: Surgeons in private practice who make their own purchasing decisions can adopt new wound closure devices faster than hospital-based surgeons working through procurement committees. For private practice, the SubQ It! SU-25 saves approximately 25 minutes per case, which can translate to one additional patient per day and roughly $6,000 in added revenue.
A study of 66 RCTs in non-obstetric surgery found that subcuticular sutures tend to produce fewer wound complications and better patient satisfaction scores than staples. For GI surgeons specifically, the evidence supports subcuticular closure as the preferred method when time and resources allow.
Bioabsorbable options now make that tradeoff far less limiting.
Final Thoughts
Subcuticular sutures offer GI surgeons better cosmetic outcomes, comparable infection rates, and improved patient satisfaction compared to metal staples. The evidence from meta-analyses, RCTs, and the Cochrane review all point in the same direction.
For a specialty where SSI rates are already elevated and every complication carries significant cost, the closure method you choose at the end of a case matters.
The practical next step is to evaluate your current closure workflow against the outcomes your patients are reporting. If you're seeing railroad-track scars, scheduling staple removal visits, or fielding complaints about cosmetic results, subcuticular closure addresses each of those pain points directly.
SubQ It! gives you subcuticular placement at a better speed with bioabsorbable fasteners that dissolve after healing. The SubQ It! SU-25 handles incisions up to 25 cm, covering the full range of GI surgery closures. Contact us today for a custom quote tailored to your practice volume and case mix.
FAQs
1. How Long Do Subcuticular Sutures Take to Absorb After GI Surgery?
Yes, absorbable subcuticular sutures dissolve on their own, typically within 60 to 180 days, depending on the material. The exact absorption timeline varies by suture type, with synthetic absorbables like polyglactin and poliglecaprone falling within that range.
2. Are Subcuticular Sutures Safe for Contaminated GI Procedures?
Yes, subcuticular sutures can be used in contaminated GI cases, though surgeons should assess each wound individually. The subcuticular technique keeps closure material beneath the skin surface, which avoids creating external puncture sites that could serve as additional entry points for bacteria.
3. Do Subcuticular Sutures Reduce Hospital Readmission Rates After Abdominal Surgery?
No clear evidence shows a direct readmission reduction from subcuticular suturing alone. However, the technique removes the need for a staple removal visit, which reduces scheduled follow-up appointments and the logistical costs associated with post-surgical callbacks.
4. Can Subcuticular Closure Be Used on Obese Patients Undergoing GI Surgery?
Yes, subcuticular closure works for obese patients, though thicker subcutaneous tissue layers require careful technique. Surgeons should ensure proper dermal-level placement to maintain wound edge alignment in patients with increased abdominal wall thickness.
5. Is Subcuticular Closure Practical for Emergency GI Procedures?
Yes, subcuticular closure can be performed in emergencies, but the added closure time may not be justified in life-threatening situations. Surgeons performing emergency laparotomies often prioritize speed, making staples or bioabsorbable stapler devices a more practical option.
6. Do Subcuticular Sutures Work for Both Laparoscopic and Open GI Incisions?
Yes, subcuticular closure applies to both laparoscopic port-site incisions and longer open-surgery incisions. For open cases with incisions up to 25 cm, bioabsorbable closure systems can place subcuticular fasteners without the time cost of manual suturing.