Skin closure is often considered routine, yet it directly influences how efficiently a procedure concludes and how the incision heals. The method chosen for staple skin closure can affect closure time, consistency, and postoperative follow-up.
As surgical volumes rise, the need for efficient and predictable closure methods continues to grow, reflected in a global wound closure market projected to reach USD 28.34 billion by 2034.
Metal staples are widely used for their speed and standardization. However, as an external method that requires removal, they entail trade-offs compared with other closure options.
In this blog, you’ll explore how surgeons evaluate staples for skin closure in 2026, including clinical indications, limitations, removal considerations, and alternatives.
What Are Staples for Skin Closure?
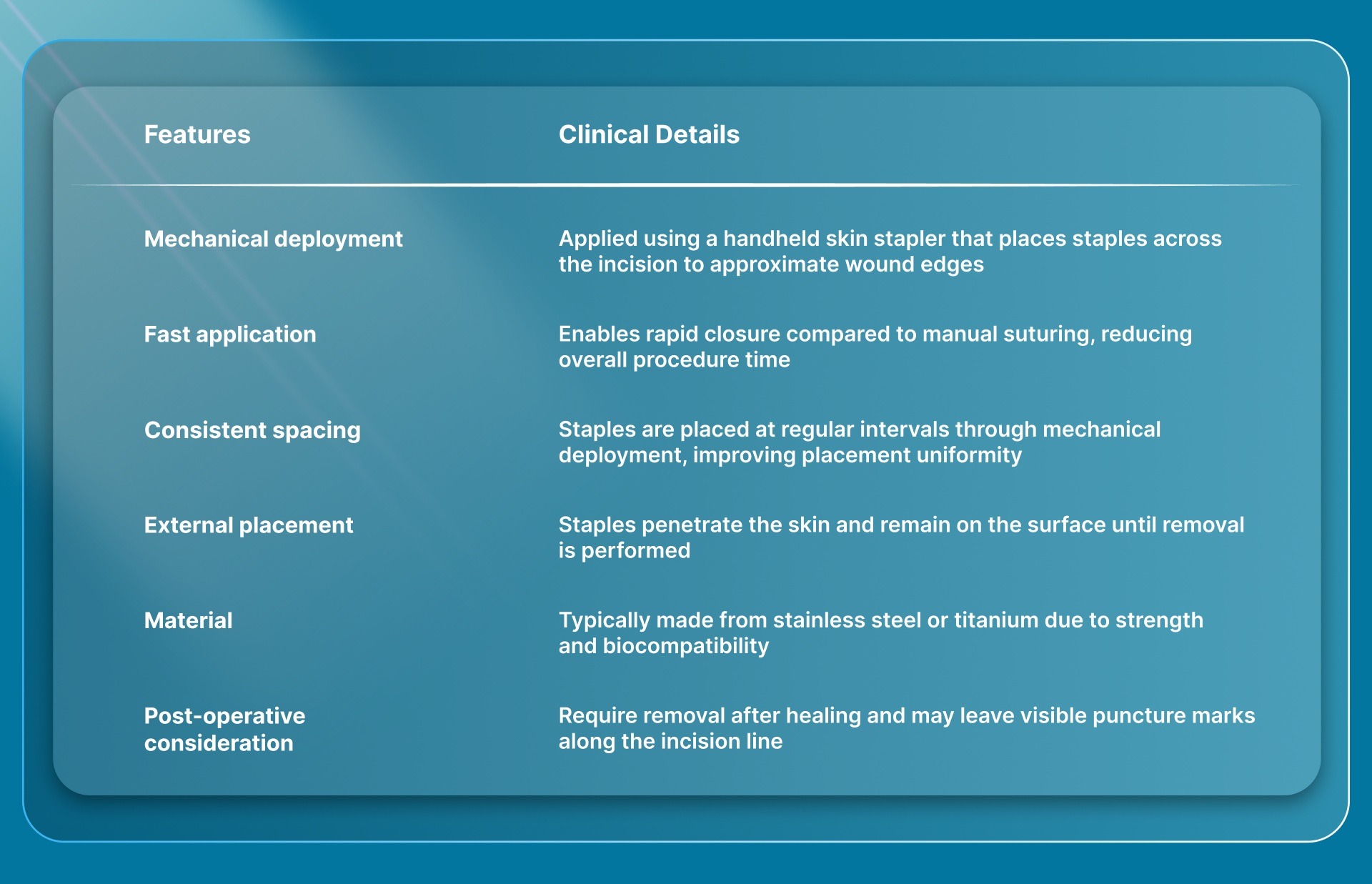
Staples for skin closure are mechanical fasteners that surgeons use to approximate skin edges at the end of a procedure. They are applied with a handheld stapler that places metal clips across the incision, enabling rapid closure in the operating room.
Each staple penetrates both sides of the skin and bends into place to hold the wound edges together until sufficient healing occurs.
Because these staples remain on the skin surface, they must be removed after a defined period, typically within 7 to 14 days, depending on the incision location and the rate of healing.
Key characteristics of staples for skin closure include:
A clear understanding of what staples for skin closure are also helps explain the clinical situations in which surgeons choose to use them.
When Do Surgeons Use Staples for Skin Closure?
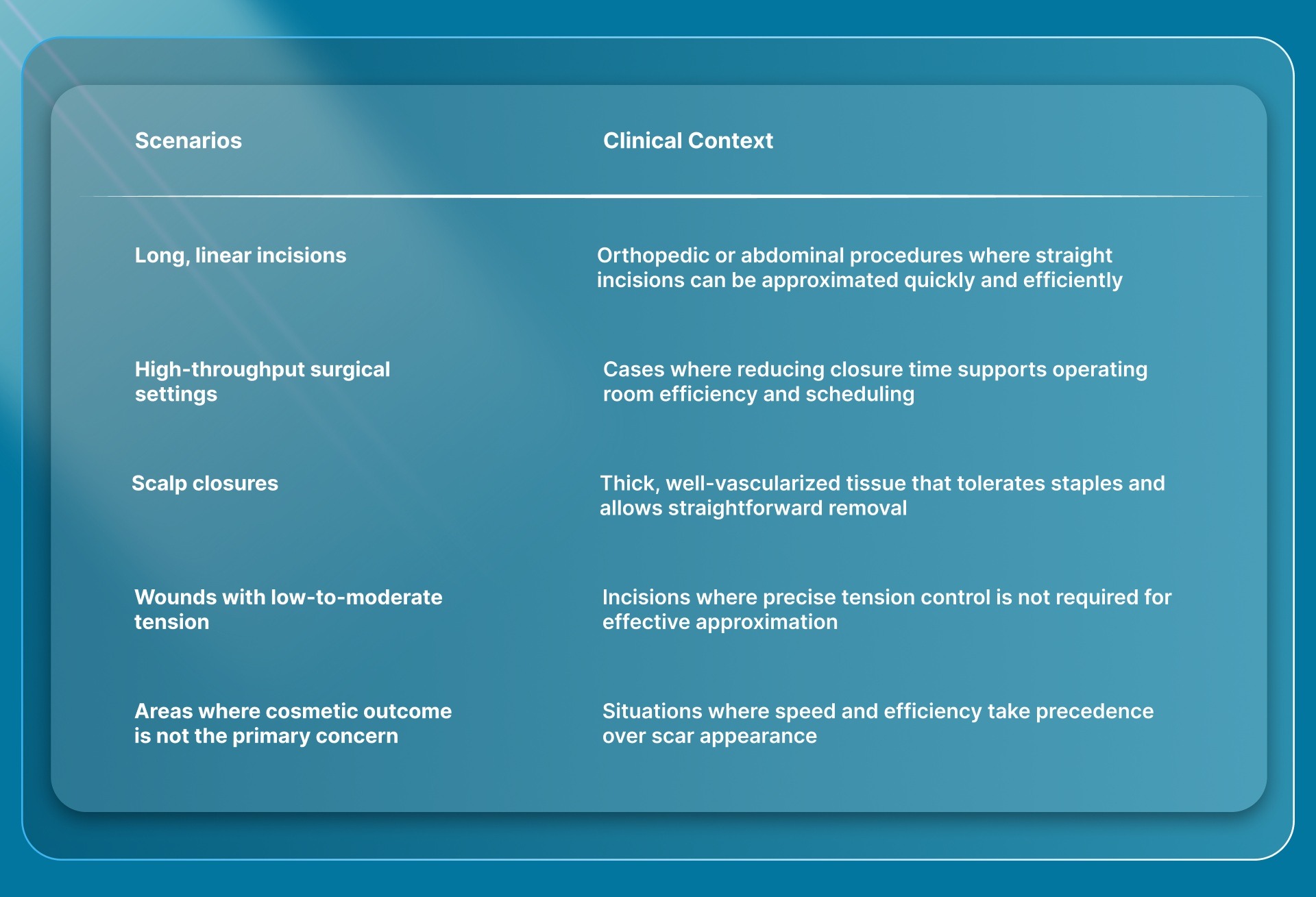
Surgeons use staples for skin closure when speed and operating room efficiency are priorities at the end of a procedure. The decision is typically made intraoperatively, based on incision type, tissue characteristics, and overall workflow requirements.
Common scenarios where staples are used for skin closure include:
In cases involving longer incisions where efficiency is critical but external staples introduce additional post-operative steps, systems like SubQ It! SU-25 provides an alternative by enabling subcutaneous, bioabsorbable closure without a removal visit.
The clinical indications for using staples also highlight the potential risks and limitations to consider.
Risks and Limitations of Staples for Skin Closure
The limitations of staples become more apparent when wound conditions require precise control beyond simple approximation.
While staples perform well in simple closures, they offer limited flexibility once deployed, which can affect outcomes in more complex or cosmetically sensitive cases.
Key risks and limitations of staples for skin closure include:
- Limited control over edge alignment: Once placed, staples do not allow fine adjustment of tissue positioning, which can affect how accurately wound edges meet
- Fixed tension application: Mechanical closure does not allow gradual tension modulation, making it less suitable for wounds requiring careful load distribution
- Challenges in high-tension areas: Incisions under stress may be more prone to separation or uneven healing when precise tension control is needed
- Dependence on placement accuracy: Misaligned placement requires removal and reapplication, adding time and disruption
- Potential for discomfort during healing: External staples can cause local irritation or sensitivity in some patients
- Additional follow-up requirement: Removal introduces an extra step in the care pathway, affecting scheduling and overall workflow
An understanding of these risks and limitations also informs decisions about the timing of staple removal and postoperative care.
Staple Removal Timelines and Post-Operative Considerations
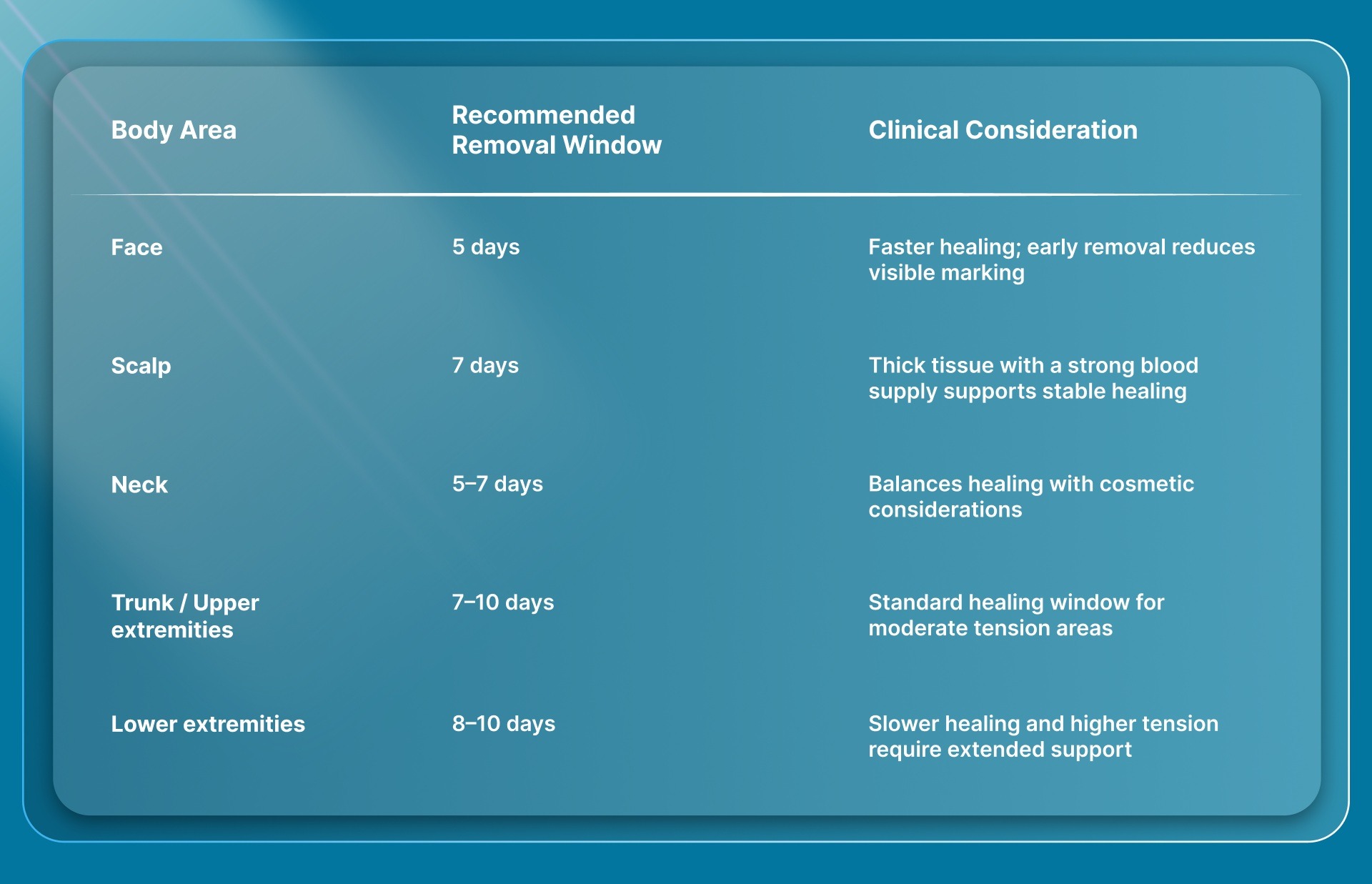
Once staples are used for skin closure, the focus shifts to timing their removal without disrupting wound healing. The removal window depends on incision location, tissue vascularity, and wound tension, all of which influence how quickly the skin regains sufficient strength.
Typical staple removal timelines by location include:
Key post-operative considerations include:
- Timing sensitivity: Early removal may risk wound separation, while delayed removal can increase the likelihood of visible marking
- Follow-up coordination: Requires scheduling a visit for removal, adding an additional step in the care pathway
- Patient compliance: Healing outcomes depend on patients returning within the recommended timeframe
- Wound monitoring: Regular assessment is needed to ensure the incision remains well-approximated before removal
- Removal procedure: Staples are removed using a dedicated instrument that disengages them from the skin
Considerations around removal timelines and follow-up care also open the discussion to alternative methods that may better suit certain clinical scenarios.
5 Key Alternatives to Staples for Skin Closure
When staples are not selected for closure, the decision shifts toward methods that offer greater control over tissue approximation or reduce external hardware on the skin.
The choice depends on the level of precision required during closure and on how the wound is expected to behave during healing.
1. Bioabsorbable Subcutaneous Fastener Systems
Bioabsorbable subcutaneous fastener systems approximate tissue beneath the skin using absorbable materials. These systems are considered in cases where internal closure is preferred, and external closure components are avoided.
2. Subcuticular Sutures (Absorbable)
Subcuticular sutures are placed within the dermal layer to approximate skin edges without leaving material on the surface. This method is used when controlled edge alignment is required and when minimizing visible surface marks is important.
3. Interrupted or Layered Sutures
Interrupted or layered sutures are used when closure requires step-by-step control across the wound. Each stitch can be adjusted independently, making this approach suitable for incisions where tension varies along the wound or where deeper layers require support.
4. Adhesive Strips
Adhesive strips are applied externally to support superficial closure in low-tension wounds. They are typically used for smaller incisions or as reinforcement after primary closure.
5. Tissue Adhesives
Tissue adhesives, such as cyanoacrylate-based glues, are used for small, clean wounds that do not require deep structural support. They form a protective layer over the incision and are suited to cases where a needle-free approach is appropriate.
Reviewing these alternatives provides a broader perspective that supports a more informed choice of the right skin closure method.
How Surgeons Can Choose the Right Skin Closure Method?
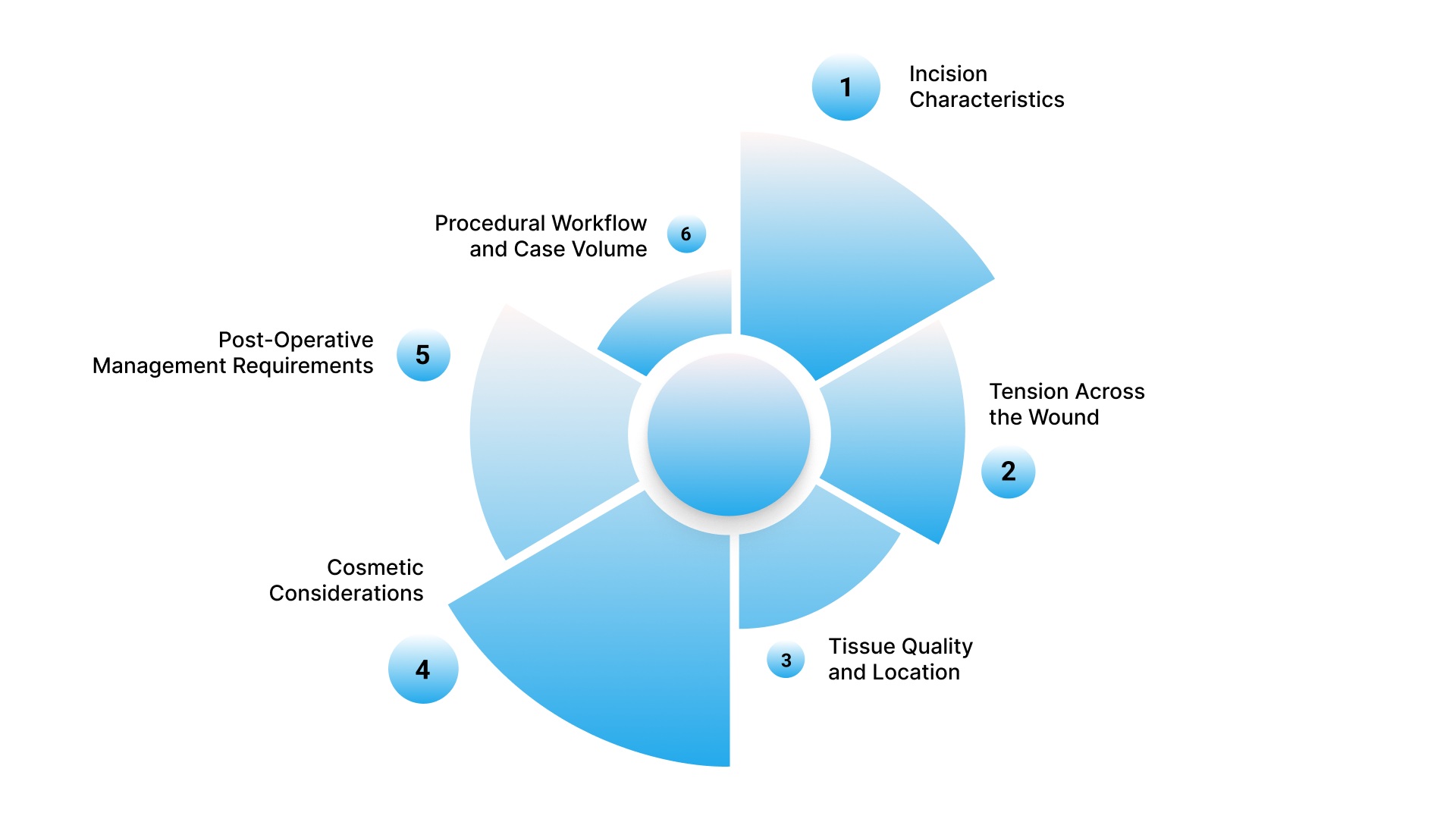
Choosing the right skin closure method is a procedural decision that directly affects wound stability, healing outcomes, and operating room workflow. The approach is typically planned before the procedure and adjusted intraoperatively based on the incision's behavior.
1. Incision Characteristics
The length, shape, and depth of the incision determine how the wound edges can be brought together. Straight, uniform incisions enable more standardized closure approaches, whereas irregular or deeper wounds require techniques that support controlled, precise approximation.
The key considerations include:
- Linear vs irregular shape: Straight incisions allow uniform closure, while irregular wounds require more controlled alignment
- Depth of incision: Deeper wounds may require layered closure rather than surface-only approximation
- Edge quality: Clean, well-defined edges are easier to approximate than uneven or traumatized tissue
2. Tension Across the Wound
Tension distribution affects how well the wound will heal. Incisions under higher or uneven tension require methods that allow gradual adjustment, while low-tension wounds can be closed using more uniform approaches.
The decision is influenced by:
- High-tension areas: Require controlled methods to distribute force across the wound
- Low-tension wounds: Can be managed with more standardized closure techniques
- Uneven tension zones: May need selective control across different segments of the incision
3. Tissue Quality and Location
Skin thickness, vascularity, and anatomical location influence how the tissue responds to closure. Different areas of the body behave differently under stress and during healing, which affects the choice of technique.
The main factors include:
- Thin or fragile skin: Requires careful handling to maintain alignment
- Thick, well-vascularized tissue: Supports more direct closure approaches
- Anatomical location: Movement and mechanical stress can affect closure stability
4. Cosmetic Considerations
Surface appearance is an important factor in many procedures, particularly in exposed areas. The selected method should align with how the incision is expected to heal and the level of visible marking that is acceptable.
This is shaped by:
- Visible areas: Require techniques that minimize surface marking
- Scar outcome expectations: Influence the choice of closure method
- Precision of edge alignment: Affects long-term cosmetic results
5. Post-Operative Management Requirements
The level of follow-up care required after closure is a practical consideration. Some methods require additional monitoring or intervention, which affects both workflow and patient management. The decision is influenced by:
- Follow-up dependency: Some methods require additional visits or interventions
- Patient compliance: Impacts how reliably post-operative care is completed
- Care pathway complexity: Simpler approaches reduce administrative and clinical burden
6. Procedural Workflow and Case Volume
In high-volume settings, closure time directly affects overall scheduling and case flow. The selected method should support efficient turnover while maintaining reliable wound approximation. Key considerations include:
- Case turnover requirements: Faster closure supports tighter scheduling
- Operating room efficiency: Closure time contributes to total procedure duration
- Consistency across cases: Predictable methods help maintain workflow stability
Final Thoughts
Effective skin closure shapes operative efficiency, post-operative management, and consistency across surgical cases. As procedural demands increase, closure methods are evaluated not only for speed but also for their reliability in real workflow conditions.
In this context, SubQ It! SU-25 is designed for longer incisions, with 25 bioabsorbable fasteners that support closure of up to 25 cm while reducing closure time by approximately 25 minutes per case.
This becomes particularly relevant in high-volume or private practice settings where closure time directly affects throughput and scheduling.
Contact us today to learn how SubQ It! SU-25 can integrate into your workflow and support more consistent, efficient closure.
FAQs
1. Are skin staples used for all types of surgical incisions?
No. Skin staples are typically used for selected incisions where rapid external closure is appropriate. The choice depends on incision shape, tissue characteristics, tension, and the level of control needed during closure.
2. Can skin staples be used in areas with significant movement?
They can be used in some mobile areas, but movement increases mechanical stress across the wound. Closure selection must account for how motion may affect wound stability and healing.
3. Do skin staples affect post-operative imaging?
Skin staples are generally safe for imaging, including MRI, but metal staples may produce artifacts depending on the material used and the type of scan performed.
4. Are skin staples used only for closing the skin layer?
Yes. In skin closure, staples are used to approximate the skin edges. When required, deeper tissue layers are closed separately using other techniques.
5. Can staple spacing affect healing outcomes?
Yes. Spacing that is either too tight or too wide can affect wound approximation and the quality of healing. Proper placement helps maintain closure without creating unnecessary stress along the incision.
6. When might staples be avoided even in a straightforward incision?
Staples may be avoided if surface appearance is a priority, follow-up removal is impractical, or the wound requires more precise control over alignment. In these cases, an alternative closure method may be more appropriate.