Introduction
Surgeons and OR teams are expected to achieve wound closures that heal reliably and minimize complications. Choosing between Monocryl vs Vicryl skin closure is a frequent, high‑impact decision in practice. Absorbable sutures are widely used, yet evidence guiding material choice can feel scattered.
A 2024 systematic review) of randomized trials in facial wound closure found that nonabsorbable and absorbable sutures produced similar rates of infection, wound dehiscence, visible scarring, and patient‑reported cosmetic outcomes. The differences were not statistically significant, supporting absorbable options as a clinical alternative when appropriate.
In this blog, we will explore the latest clinical evidence on Monocryl vs Vicryl skin closure. We will compare how each performs across surgical contexts. We will also provide practical guidance to help surgical teams make evidence‑based closure decisions.
TL;DR
- Clinical Outcomes: Both sutures show similar infection, dehiscence, and cosmetic results.
- Monocryl: Smooth monofilament; ideal for cosmetic, subcuticular, and low-tension closures; reduces tissue trauma and early post-op pain.
- Vicryl: Braided; strong knot security; suited for multi-layered or moderate-tension internal tissue closures.
- Efficiency & Comfort: Monocryl minimizes extrusion and inflammation; Vicryl ensures reliable tissue support with slightly slower handling.
- Evidence-Based Choice: Selecting suture by tissue type, closure tension, and patient factors optimizes healing and reduces complications.
What is Monocryl?
Monocryl is a synthetic, absorbable monofilament suture made of poliglecaprone 25. It is used to close surgical wounds and internal tissues, gradually dissolving in the body so removal isn’t required.
- Type: Absorbable, monofilament suture
- Material: Poliglecaprone 25 (synthetic polymer)
- Purpose: Provides temporary support for wound healing
What is Vicryl?
Vicryl is a synthetic, absorbable braided surgical suture made of polyglactin 910—a copolymer of glycolide and l‑lactide. It gradually loses tensile strength over the first few weeks after placement and is fully absorbed by hydrolysis in about 60–90 days, so it typically does not need removal.
- Type: Absorbable, braided suture
- Material: Polyglactin 910 copolymer (glycolide and lactide)
- Purpose: Provides temporary wound support in soft tissue approximation and ligation
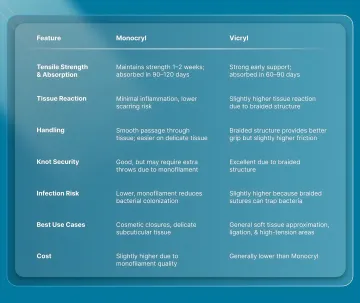
Monocryl or Vicryl? How to Pick the Right Absorbable Suture for Surgery
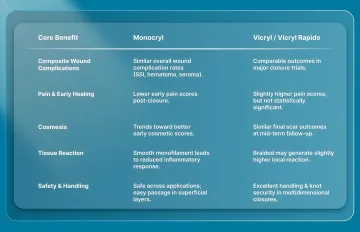
Monocryl and Vicryl each have strengths for different types of closures. The table below shows when one might be preferred over the other.
Real-World Scenarios Where Surgeons Choose Monocryl or Vicryl
Monocryl and Vicryl each have their place in the OR. Choice comes down to tissue type, closure tension, and how the suture behaves during healing. The following are some common real-world applications for each suture:
Monocryl Applications
- Subcuticular Skin Closures
- Often used for cosmetic closures in areas like the face, neck, or hands.
- Its smooth monofilament design reduces tissue trauma, lowers infection risk, and leaves minimal scarring.
- Delicate Soft Tissue Approximation
- Preferred in pediatric surgeries or delicate organs, where gentle handling is critical.
- Provides temporary support during early healing without leaving long-term foreign material.
- Internal Low-Tension Closures
- Suitable for subcutaneous or abdominal closures where wound tension is low.
- Minimizes tissue reaction and adhesion formation while maintaining support during healing.
Vicryl Applications
- Internal Soft Tissue Approximation
- Ideal for fascia, subcutaneous tissue, and internal organ repair where absorbable support is needed.
- Braided structure provides good knot security without leaving permanent material.
- Moderate-Tension Closures
- Suitable for soft tissue layers where tissues need temporary support.
- Maintains integrity through early healing but is fully absorbed within 60–90 days.
- Soft Tissue Ligation
- Used to tie small to medium-sized vessels or tissue bundles during surgery.
- Slightly higher tissue reaction is acceptable in deeper layers, as the cosmetic outcome is less critical.
6 Evidence-Based Benefits of Monocryl vs Vicryl for Surgeons
Beyond basic suture properties, Monocryl and Vicryl offer benefits that directly impact intraoperative efficiency, post-operative outcomes, and surgeon decision-making:
Monocryl vs Vicryl: What Closure Challenges Do Surgeons Face?
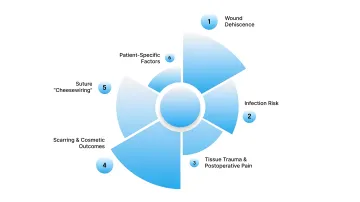
Even with ideal suture selection, surgical teams can face technical or patient-related complications. Anticipating these issues and knowing practical solutions ensures safer, faster, and more predictable wound closure.
1. Wound Dehiscence
- Problem: High-tension closures or inadequate layer support can lead to wound separation.
- Solution:
- Use layered closure techniques to distribute tension.
- Reinforce high-tension areas with deep sutures.
- Evidence: Monocryl loses tensile strength over 1–2 weeks; matching closure strategy to tissue healing reduces dehiscence
2. Infection Risk
- Problem: Braided Vicryl can trap bacteria, increasing infection potential.
- Solution:
- Minimize tissue handling.
- Irrigate thoroughly, especially in contaminated or high-risk wounds.
- Evidence: Monofilament sutures show lower bacterial adherence in surgical studies
3. Tissue Trauma & Postoperative Pain
- Problem: Friction and drag from suture passage can increase inflammation and discomfort.
- Solution:
- Use monofilament sutures in delicate tissues.
- Pass sutures deliberately in wet or slippery tissue.
- Evidence: Smooth monofilament reduces tissue trauma and early postoperative pain
4. Scarring & Cosmetic Outcomes
- Problem: Excessive tissue tension or reaction can worsen scar formation.
- Solution:
- Use Monocryl for subcuticular or facial closures.
- Avoid overly tight bites that compress tissue.
- Evidence: Monofilament sutures are associated with reduced hypertrophic scarring in cosmetic procedures
5. Suture “Cheesewiring”
- Problem: Over-tensioning can cause the suture to cut through delicate tissue.
- Solution:
- Choose an appropriate suture size for tissue strength.
- Avoid excessively tight knots.
- Evidence: Balanced tension preserves tissue integrity and promotes reliable healing
6. Patient-Specific Factors
- Problem: Comorbidities like diabetes or poor vascularity can slow healing.
- Solution:
- Consider supplemental deep closure or layered reinforcement.
- Closely monitor high-risk patients for early signs of complications.
- Evidence: Tailored suture strategies reduce delayed healing in compromised tissues
Final Thoughts
Monocryl and Vicryl each offer reliable, absorbable solutions for skin and soft tissue closure, with unique strengths depending on tissue type, closure tension, and surgical context. While suture selection alone doesn’t guarantee outcomes, using the right material in the right scenario can reduce complications, improve healing, and enhance patient satisfaction.
For reliable and predictable skin and superficial tissue closure, bioabsorbable subcuticular systems like SubQ It! offer an effective alternative. By eliminating staple removal and reducing technique variability, they streamline procedures while supporting optimal healing.
Integrating SubQ IT! into your workflow can improve efficiency, minimize complications, and enhance patient outcomes. Contact the SubQ It! team to see how your practice can benefit.
FAQs
1. Monocryl vs Vicryl: Which Suture Should I Use for Cosmetic Skin Closures?
Monocryl’s smooth monofilament design minimizes tissue trauma and scarring, making it ideal for facial subcuticular skin closure, while Vicryl is better for deeper or higher-tension internal layers.
2. How Long Do Monocryl and Vicryl Sutures Last in the Body?
Monocryl maintains strength for 1–2 weeks and is fully absorbed in 90–120 days. Vicryl provides stronger early support and absorbs completely in 60–90 days, suitable for internal tissue repair.
3. Does Suture Choice Affect Postoperative Pain and Healing?
Yes. Monocryl generally causes lower early postoperative pain and promotes faster perceived healing in delicate closures, whereas Vicryl ensures reliable support but may slightly increase early discomfort.
4. When Should Vicryl Be Preferred Over Monocryl?
Vicryl’s braided structure offers excellent knot security, making it the preferred choice for multi-layered, moderate-tension, or internal soft tissue closures.
5. What Patient Factors Influence Suture Selection?
Patient comorbidities such as diabetes, poor circulation, or compromised tissue healing may require careful suture selection and layered closure techniques to reduce complications.
6. Can Absorbable Sutures Reduce Infection and Tissue Trauma?
Yes. Monocryl’s monofilament design lowers bacterial adherence and tissue reaction, reducing infection risk and inflammation, while Vicryl’s braided design may slightly increase these risks in superficial closures.
7. What Are Common Closure Complications and How to Avoid Them?
Complications include wound dehiscence, scarring, suture “cheesewiring,” and infection. Solutions include using appropriate suture type and size, layered closure, gentle tissue handling, and choosing Monocryl for delicate cosmetic areas.
8. Do I need to remove Monocryl or Vicryl sutures?
Neither requires removal—both are absorbed by the body. This advantage extends to bioabsorbable closure systems like SubQ It!, which combines the speed of traditional staplers with absorbable subcuticular fasteners, eliminating removal appointments entirely.