Introduction: Understanding Prolene Sutures in Modern Wound Closure
Choosing the right suture material directly impacts wound healing outcomes and patient satisfaction. Surgeons face critical decisions daily: Will this closure minimize scarring? Can the patient return reliably for removal? Is infection risk a concern?
Prolene (polypropylene) sutures have served as a workhorse in surgical wound closure for decades, offering predictable performance and excellent tensile strength. Proper use requires understanding when Prolene performs best, mastering its unique handling characteristics, and recognizing when modern alternatives may serve patients better.
This guide covers practical techniques for Prolene use, optimal clinical scenarios, and how emerging bioabsorbable closure systems are reshaping surgical practice—particularly for minimally invasive procedures where speed and cosmesis both matter.
TLDR:
- Monofilament structure provides superior infection resistance with significantly lower bacterial colonization
- Use a surgeon's knot with 3-4 throws to counter material memory and slipperiness
- Remove within 5-7 days (face), 7-10 days (trunk), or 10-14 days (extremities) to prevent scarring
- Bioabsorbable systems eliminate removal visits while closing 7X faster than sutures
- Ideal for contaminated wounds, high-tension closures, and patients who can return for removal
What is Prolene? Material Properties and Characteristics
Understanding Polypropylene as a Suture Material
Prolene is a synthetic, non-absorbable, monofilament suture manufactured from polypropylene polymer. This crystalline structure provides long-term tissue support without degradation.
Its smooth, unbraided surface distinguishes it from multifilament alternatives.
Key physical properties include:
- Minimal tissue reactivity: Prolene demonstrates the lowest bacterial colonization rates compared to Vicryl Plus, Monocryl, and silk (p < 0.001)
- High tensile strength: Maintains structural integrity indefinitely in vivo without degradation
- Memory characteristics: Retains package shape and tends to spring back, requiring specific handling techniques
- Inflammatory response: Causes minimal acute reaction, followed by gradual fibrous encapsulation
Key Advantages of Prolene
Prolene offers distinct clinical advantages:
- Infection resistance: The monofilament structure prevents bacterial colonization within braided fibers, reducing plaque formation and microbial adherence
- Predictable removal: Sutures remove cleanly without fragmentation when timing is appropriate, allowing surgeons to optimize cosmetic outcomes
- Knot security: Provides excellent security when tied correctly using surgeon's knots, despite requiring precise technique due to low friction
- Superior cosmetic potential: Produces minimal scarring when removed at optimal timing (typically 7-14 days depending on location)
The smooth surface makes Prolene ideal for contaminated or high-risk wounds where infection prevention is critical.
Handling Characteristics and Challenges
While Prolene offers clinical benefits, it presents unique handling challenges:
Memory retention: Prolene retains its coiled package shape, causing the suture to spring back during placement. Straightening the material before use and maintaining firm control prevent handling problems.
Slippery surface: The smooth monofilament has a lower friction coefficient than braided sutures. Standard knots slip easily—surgeon's knots (double first throw) are essential for security.
Practice requirements: These characteristics require mastery but offer advantages once learned. The smooth surface passes through tissue with minimal drag, particularly valuable in contaminated fields where tissue planes may be inflamed or friable.
When to Use Prolene Sutures: Indications and Best Applications
Ideal Clinical Scenarios for Prolene
Primary indications:
- Contaminated or infected wounds where the monofilament structure resists bacterial involvement and minimizes sinus formation
- High-tension areas requiring indefinite tensile strength retention under mechanical stress
- Vascular anastomoses where non-thrombogenic properties prevent clot formation
- Cosmetically sensitive areas requiring precise wound edge approximation
- Device implantations (pacemakers, defibrillators), where infection prevention is critical
- Reopened or complicated wounds where absorbable materials pose an increased risk
Prolene excels when infection control outweighs convenience considerations. It also requires patients who can reliably return for removal.
When to Avoid or Reconsider Prolene
While Prolene offers clear advantages in infection control, certain situations favor absorbable alternatives:
Contraindications and cautions:
- Pediatric patients who may not tolerate removal procedures
- Patients unlikely to return for follow-up, risking prolonged retention and scarring
- Remote anatomic locations where removal is technically difficult
- Patients who strongly prefer avoiding removal appointments
Situations favoring absorbables: Despite Prolene's infection resistance, absorbable sutures prove non-inferior for wound infection, dehiscence, and cosmetic outcomes in many applications according to a meta-analysis of 19 randomized controlled trials.
Patient Selection Considerations
Decision factors:
- Pediatric and geriatric patients may have different tolerances for removal procedures
- Facial wounds demand early removal (5-7 days) to avoid permanent scarring
- Realistically assess whether the patient will return at the optimal timing
- Joint proximity affects tension and required support duration
- Contaminated wounds, diabetes, and immunosuppression favor monofilament materials
Patient communication: Explain the need for removal, optimal timing, and expected cosmetic outcomes. Set clear expectations about follow-up requirements and potential consequences of delayed removal.
Handling Tips for Prolene Sutures: Techniques for Optimal Results
Preparation and Initial Handling
Managing Prolene's memory:
- Gently straighten the suture before use by running it between gloved fingers
- Maintain gentle but firm control throughout placement
- Work with the material's natural curve rather than fighting it
Suture size selection by region:
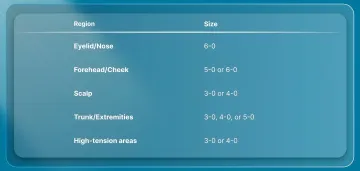
- Face (eyelid, nose): 6-0
- Face (forehead, cheek): 5-0 or 6-0
- Scalp: 3-0 or 4-0
- Trunk and extremities: 3-0, 4-0, or 5-0
- High-tension areas: 3-0 or 4-0
Needle selection: Reverse cutting needles work best for skin, with three-eighths curvature appropriate for most traumatic lacerations.
Knotting Techniques for Prolene
Prolene's smooth surface and low friction coefficient allow standard square knots to slip under tension. Use a surgeon's knot instead:
- First throw: Double wrap (2 loops around) to create friction
- Second throw: Single wrap in the opposite direction
- Third throw: Single wrap, maintaining square configuration
- Configuration: 2-1-1 for most applications, 3-1-1 for high-tension areas
Once the knot is complete, focus on tension. Approximate wound edges without strangulation. Overly tight sutures cause tissue ischemia (reduced blood flow) and "train track" scarring. Test knot security gently before cutting tails.
Troubleshooting knot slippage:
- Ensure flat, square ties (not granny knots)
- Add additional throws for polypropylene (4-5 total)
- Leave adequate tail length (3-4mm) to prevent unraveling
- Consider instrument ties for better control in slippery conditions
Suture Placement Strategies
Bite Depth and Spacing
Proper bite technique varies by location:
- Depth: 2-3mm from wound edge for facial wounds, 4-5mm for trunk/extremities
- Spacing: 2-3mm apart on face, 4-5mm on body
- Symmetry: Enter and exit at the same depth on both sides
Interrupted vs. Continuous Techniques
Interrupted suturing is standard for Prolene. It allows individual adjustment and minimizes total suture loss if one breaks.
Continuous subcuticular closure is less common with Prolene but faster. Continuous sutures show lower dehiscence rates (OR 0.16) in a systematic review, though they require careful tension management.
Achieving even approximation:
- Evert wound edges slightly (they flatten during healing)
- Avoid "stepping" where edges overlap at different heights
- Use forceps to manipulate tissue, not the suture itself
- Place deep dermal sutures first in high-tension closures to reduce superficial suture load
Removal Timing and Technique
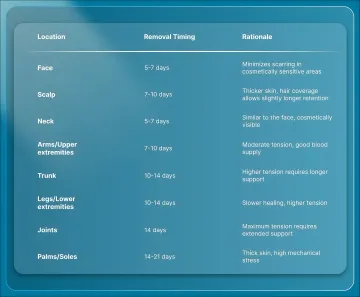
Optimal removal by anatomic region:
| Location | Removal Timing | Rationale |
|---|---|---|
| Face | 5-7 days | Minimizes scarring in cosmetically sensitive areas |
| Scalp | 7-10 days | Thicker skin, hair coverage allows slightly longer retention |
| Neck | 5-7 days | Similar to the face, cosmetically visible |
| Arms/Upper extremities | 7-10 days | Moderate tension, good blood supply |
| Trunk | 10-14 days | Higher tension requires longer support |
| Legs/Lower extremities | 10-14 days | Slower healing, higher tension |
| Joints | 14 days | Maximum tension requires extended support |
| Palms/Soles | 14-21 days | Thick skin, high mechanical stress |
Removal technique:
- Clean the area with an antiseptic
- Grasp the knot with forceps and lift gently
- Cut the suture on one side close to the skin
- Pull smoothly in the direction parallel to the wound
- Avoid jerking motions that cause patient discomfort
Surgeons must adhere to anatomic-specific removal windows to prevent train-track scarring and optimize cosmetic outcomes.
Prolene vs. Alternatives: Choosing the Right Suture Material
Prolene vs. Absorbable Sutures (Vicryl, Monocryl)
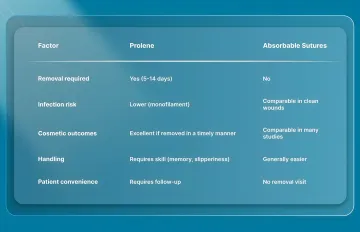
Key comparison factors:
| Factor | Prolene | Absorbable Sutures |
|---|---|---|
| Removal required | Yes (5-14 days) | No |
| Infection risk | Lower (monofilament) | Comparable in clean wounds |
| Cosmetic outcomes | Excellent if removed in a timely manner | Comparable in many studies |
| Handling | Requires skill (memory, slipperiness) | Generally easier |
| Patient convenience | Requires follow-up | No removal visit |
Clinical evidence shows significant differences. A retrospective study of distal radius fractures found that interrupted Prolene sutures resulted in higher pain scores (mean 1.48 vs 1.37), worse cosmetic outcomes (POSAS scores 38.41 vs 29.03, p=0.000033), and higher complication rates (88.9% vs 36.8%) compared to continuous subcuticular Monocryl.
Absorbable sutures work better in several scenarios:
- Pediatric cases where removal causes distress
- Areas where removal is technically difficult
- Patients with uncertain follow-up compliance
- Patient preference to avoid removal procedures
- Situations where convenience outweighs marginal infection risk differences
Prolene vs. Staples
Both options deploy rapidly (roughly 7 seconds each), but staples require removal and produce inferior cosmetic outcomes.
Infection risk varies by procedure type:
- Hip arthroplasty: Staples carry 2.5X higher SSI risk (RR 2.51; 95% CI 1.15-5.50) compared to sutures
- Lower extremity bypass: Staples associated with 57% higher SSI odds (OR 1.57; 95% CI 1.21-2.04)
- Knee arthroplasty: No significant difference between staples and sutures
Cosmetically, staples pierce external skin and leave visible entry/exit marks ("train tracks"). Prolene produces superior results when removed appropriately.
While staples cost less per unit, overall healthcare costs run higher due to removal appointments and increased infection rates in certain procedures.
Modern Alternatives: Bioabsorbable Closure Systems
Beyond choosing between traditional options, surgeons now have access to bioabsorbable subcuticular closure systems that combine speed with improved cosmesis by placing fasteners entirely beneath the skin surface.
The SubQ It! system offers distinct advantages:
- Deploys bioabsorbable fasteners subcutaneously (external skin never pierced)
- Achieves 7X faster closure than manual sutures
- Eliminates removal requirements—fasteners absorbed by body after healing
- Particularly valuable for laparoscopic and minimally invasive incisions
- FDA-cleared for abdominal, thoracic, gynecologic, orthopedic, and plastic/reconstructive surgery
Pre-loaded staplers deploy bioabsorbable fasteners into dermal tissue using small needles that immediately retract. The fasteners' barbed design engages tissue away from the wound edge, maintaining approximation through tensile strength of connecting bridges while minimizing ischemia.
These systems offer compelling advantages for trocar closures, laparoscopic port sites, and other small incisions where traditional methods leave visible scarring or require inconvenient removal visits.
Anatomic Region Recommendations: Where Prolene Works Best
Face and Scalp Considerations
Facial wounds: Fine Prolene (5-0 or 6-0) provides excellent results when removed within 5-7 days. The low tissue reactivity and smooth removal minimize scarring in cosmetically critical areas.
Timing is critical: Facial skin heals rapidly with excellent blood supply. Removal by day 7 prevents epithelialized suture tracks while providing adequate wound support.
For areas of highest cosmetic concern (periorbital, nasal tip), some surgeons prefer subcuticular absorbable sutures to eliminate removal trauma entirely, especially for anxious patients or children.
Scalp wounds: Larger Prolene (3-0 or 4-0) works well due to thicker skin and hair coverage that conceals any minor scarring. Removal at 7-10 days balances wound support with scar prevention.
Trunk and Extremities
Trunk closures: Use 3-0 or 4-0 Prolene with removal at 7-10 days for most applications. Higher-tension areas (lower abdomen, back) may require 10-14-day retention.
Extremity considerations:
- Standard extremity wounds: 10-14-day removal
- Over joints: 14 days minimum due to constant motion and tension
- Distal extremities: Slower healing requires longer support
- Orthopedic closures: Continuous subcuticular absorbable techniques may be preferable where tension is moderate and cosmesis matters (distal radius fracture studies showed inferior outcomes with interrupted Prolene)
- Consider patient mobility and mechanical stress on the wound
Surgical Specialty Considerations
Orthopedic procedures:
- Hip arthroplasty: Strongly prefer Prolene over staples (2.5X lower infection risk)
- Knee arthroplasty: Prolene and staples show comparable infection rates
- Consider subcuticular absorbable alternatives for cosmetically visible areas
Minimally invasive and laparoscopic surgery: Bioabsorbable subcuticular systems offer significant advantages for trocar closures and port sites. These systems combine rapid deployment with superior cosmesis and eliminate removal visits entirely.
Cardiac pacing and device implantation: Prolene's infection resistance and non-absorbable nature make it preferred for pocket closures where device infection carries catastrophic consequences.
Vascular surgery: Prolene remains the gold standard for anastomoses due to non-thrombogenic properties and permanent tensile strength.
Common Mistakes and Troubleshooting with Prolene Sutures
Knotting Errors and Solutions
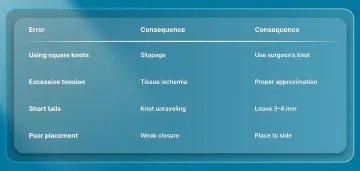
Common knotting errors include:
- Using standard square knots (inadequate throws) leading to slippage
- Excessive tension causes tissue strangulation and reduced blood flow
- Improper knot placement (too close or too far from the wound edge)
- Cutting tails too short (less than 3mm), allowing unraveling
To prevent these issues:
- Use surgeon's knot consistently (2-1-1 or 3-1-1 configuration)
- Test knot security gently before cutting by tugging parallel to the wound
- Position knots to one side of the wound, not directly over the incision line
- Leave 3-4mm tails for security
- Add extra throws (4-5 total) for high-tension areas
Wound Edge Problems
Beyond the knotting technique, proper wound edge alignment is critical for optimal cosmetic outcomes.
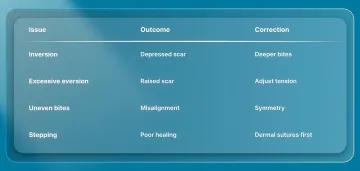
Eversion and inversion issues affect scar appearance:
- Inversion (edges roll inward): Causes a depressed scar; correct by taking deeper bites or placing dermal sutures first
- Eversion (edges protrude outward): Mild eversion is ideal (flattens during healing); excessive eversion causes a raised scar
Uneven approximation results from asymmetric bites. Enter and exit at identical depths on both sides. Use skin hooks or forceps to manipulate tissue, not the needle.
"Stepping" of tissue planes occurs when dermal and epidermal layers don't align. Place deep dermal sutures first to approximate deeper layers before surface closure.
High-Tension Closure Management
When wound tension threatens proper edge alignment, a layered approach works best:
- Place deep dermal sutures (absorbable) to reduce tension on the superficial layer
- Use larger Prolene (3-0 or 4-0) for superficial interrupted sutures
- Space sutures closer together (4-5mm) to distribute tension
- Avoid over-tightening any single suture
For extremely high-tension wounds, consider retention sutures, delayed closure, or negative pressure wound therapy rather than relying solely on tight superficial sutures. Bioabsorbable subcuticular closure systems like SubQ It! offer an alternative approach that distributes tension beneath the skin surface while maintaining closure speed, eliminating many common suturing challenges.
Suture Material Management
Memory control: Remove the suture from the package well before use and allow it to straighten naturally. Store in an open position on the sterile field.
Preventing tangles: Handle one suture at a time. Keep unused sutures organized in separate areas of the sterile field. Use suture organizers or magnetic mats for complex closures.
Maintaining sterility: Avoid dragging suture across non-sterile surfaces. If contamination occurs, discard and use fresh material—infection risk outweighs material cost.
Frequently Asked Questions
1. How long should Prolene sutures stay in before removal?
Timing varies by anatomic location: face 5-7 days, scalp and trunk 7-10 days, extremities 10-14 days, and over joints 14 days. Earlier removal generally produces better cosmetic outcomes by preventing epithelialized suture tracks that create permanent "train track" marks.
2. Is Prolene better than absorbable sutures for skin closure?
Prolene offers superior infection resistance and excellent cosmetic outcomes when properly timed for removal. Absorbable sutures eliminate removal visits and prove non-inferior for wound healing, making them preferable when follow-up is uncertain.
3. Does Prolene cause more scarring than other suture materials?
Prolene causes minimal scarring due to low tissue reactivity. However, leaving it in too long or applying excessive tension creates "train track" marks. Proper technique and timely removal produce excellent cosmetic results.
4. Can Prolene sutures be used on the face?
Fine Prolene (5-0 or 6-0) is excellent for facial wounds when removed within 5-7 days. Some surgeons prefer subcuticular absorbable sutures for areas of greatest cosmetic concern to eliminate removal trauma, particularly in pediatric or anxious patients.
5. What are the disadvantages of using Prolene for skin closure?
Requires patient return for removal, difficult handling due to memory and slipperiness, and can leave suture marks if removal is delayed or tension is excessive. Less suitable when patient follow-up is uncertain.
6. Are there faster alternatives to Prolene sutures for skin closure?
Staples deploy as quickly as Prolene but have inferior cosmetic outcomes and higher infection rates in certain procedures. Bioabsorbable subcuticular closure systems like SubQ It! offer speed advantages (up to 7X faster than manual sutures) with superior cosmesis and no removal requirement, particularly valuable for laparoscopic and minimally invasive procedures.