In high-tension surgical scenarios, every choice carries weight. When wounds span joints or involve tendons and fascia, the risk of repair failure rises if the closure material cannot withstand mechanical stress. This uncertainty can prolong procedures, increase follow-up interventions, and complicate patient recovery.
The right closure strategy addresses these challenges by maintaining strength where it matters most, reducing the likelihood of dehiscence, and supporting optimal healing. Yet achieving this requires balancing tensile support, tissue response, and patient comfort while ensuring efficiency in the operating room.
This blog provides a comprehensive guide to non-absorbable sutures, covering material types, clinical use cases, removal best practices, and modern alternatives that simplify care without compromising strength.
Key Takeaways
- Non-absorbable sutures provide consistent, long-term strength, making them essential in high-tension and slow-healing tissues.
- Material and structure choices directly impact strength, infection risk, handling, and tissue response.
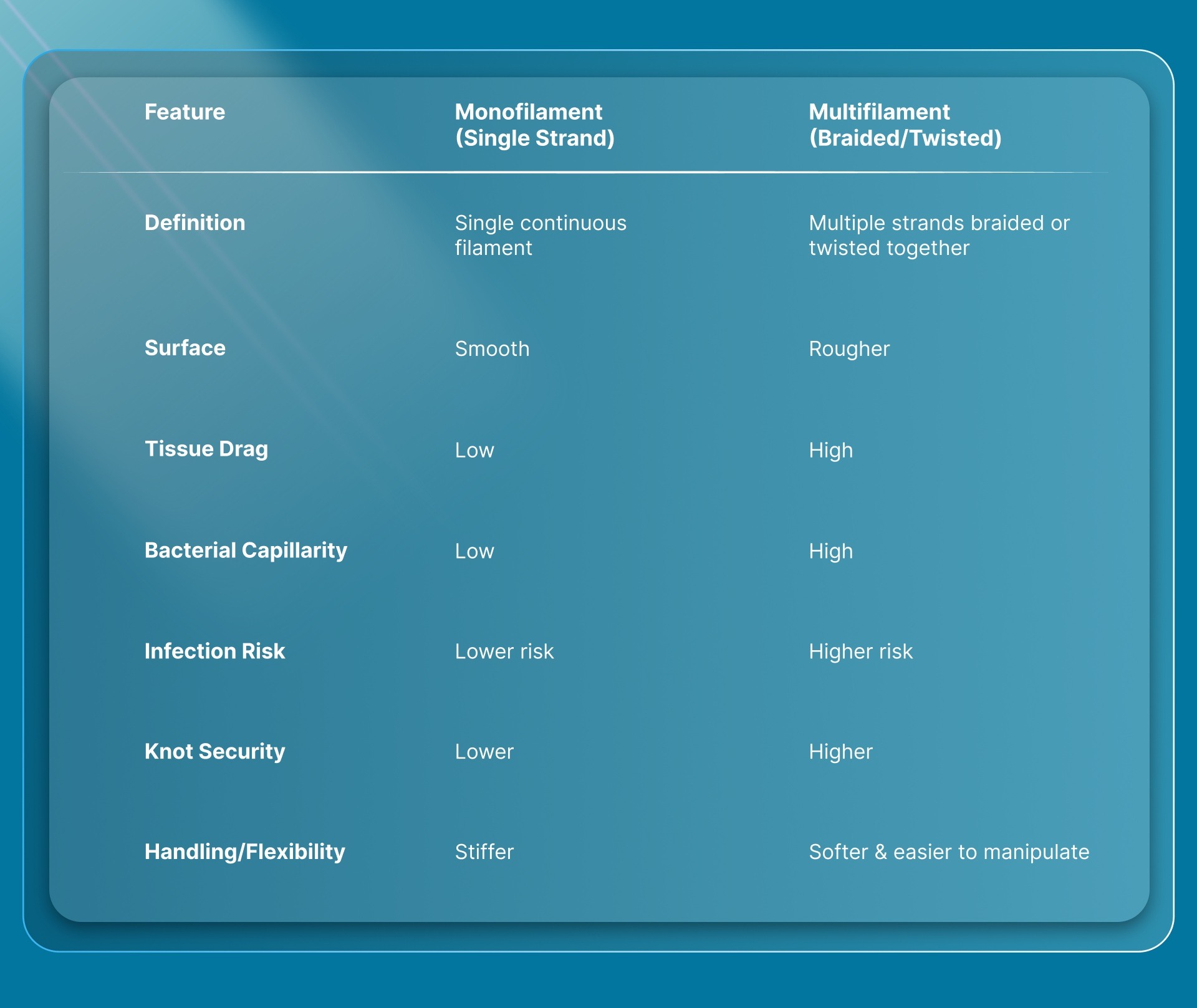
- Monofilament reduces infection risk, while multifilament improves handling and knot security.
- Widely used across skin, vascular, orthopedic, and implant fixation, where durability is critical.
- Limitations like removal, workflow burden, and cosmetic concerns are driving a shift toward more efficient closure approaches.
What Are Non‑Absorbable Sutures?
Non‑absorbable sutures are strands of suture material that are resistant to absorption and do not degrade in mammalian tissue after implantation. This distinguishes them from absorbable sutures, which progressively lose strength and are eventually absorbed by the body.
The basic structural categories related to non‑absorbable sutures include:
- Monofilament: made of a single strand of material
- Multifilament: braided or woven from multiple strands
6 Essential Non‑Absorbable Suture Materials Surgeons Use
Non‑absorbable suture materials can be natural or synthetic and vary in structure (monofilament vs. braided) and material properties.
The following are the common types of non‑absorbable suture materials:
1. Natural Non‑Absorbable Sutures
These are derived from natural substances and are not significantly broken down in tissues.
Silk
- Source: Protein fibers from silkworm larvae.
- Structure: Braided multifilament.
- Features: Excellent handling and knot security; however, it causes a moderate tissue reaction and has higher capillarity (can harbor bacteria).
2. Synthetic Non‑Absorbable Sutures
Synthetic materials are commonly preferred because they tend to be strong, less reactive, and more predictable.
a. Monofilament Synthetic Sutures
These are single‑strand threads with minimal tissue drag and lower infection risk.
Polypropylene (e.g., Prolene)
- Highly inert; retains tensile strength indefinitely.
- Smooth surface → easier passage through tissue.
Polybutester (e.g., Novafil)
- Elastic, good handling, and strong.
- It combines the advantages of polypropylene and polyester.
b. Multifilament Synthetic Sutures
These are braided for better handling, though they may have higher capillarity.
Polyester (e.g., Mersilene, Ethibond, Surgilene)
- Braided multifilament may be coated for smoother passage.
- Very high tensile strength; retains strength long term.
Nylon (e.g., Ethilon, Nurolon)
- Available as both monofilament and multifilament.
- Good strength; monofilament form has lower tissue reactivity.
3. Metal Sutures
Strong and inert, metal sutures are used in specific surgical contexts.
Stainless Steel
- Features: Extremely tensile strength and minimal tissue reaction.
Monofilament vs Multifilament: Which Non‑Absorbable Works Best?
The following comparison table shows the key differences between monofilament and multifilament non‑absorbable suture structures:
Monofilament Sutures
Monofilament sutures are made of a single smooth strand of material. They are often chosen when low infection risk and smooth tissue passage matter most.
Pros
- Low tissue drag: Smooth surface causes minimal trauma as it passes through tissue.
- Lower infection risk: Less fluid wicking and fewer spaces for bacteria to hide compared with braided sutures.
- Reduced tissue reaction: Less surface area contacting tissue means less inflammation.
Cons
- Poorer knot security: High memory and smooth surface make secure knots harder to form.
- Challenging handling: Often stiffer and less flexible than braided (multifilament) sutures.
Multifilament Sutures
Multifilament sutures consist of multiple strands braided or twisted together. They are typically used where handling comfort and reliable knots are a priority.
Pros
- Better handling: Braided structure makes them more flexible and easier to manipulate.
- Improved knot security: The texture and friction between fibers help knots hold more reliably.
Cons
- Higher tissue drag: Braided surface increases friction during passage.
- Greater infection potential: Fluid wicking and spaces between fibers can trap bacteria, increasing infection risk.
- More tissue reaction: Larger surface area and more material can provoke a stronger inflammatory response.
Where Do Surgeons Choose Non‑Absorbable Sutures?
Non‑absorbable sutures are used in situations where long‑term mechanical support and wound strength are essential and where the sutures are intended to remain in place indefinitely unless removed. Here are the following:
Common Clinical Uses
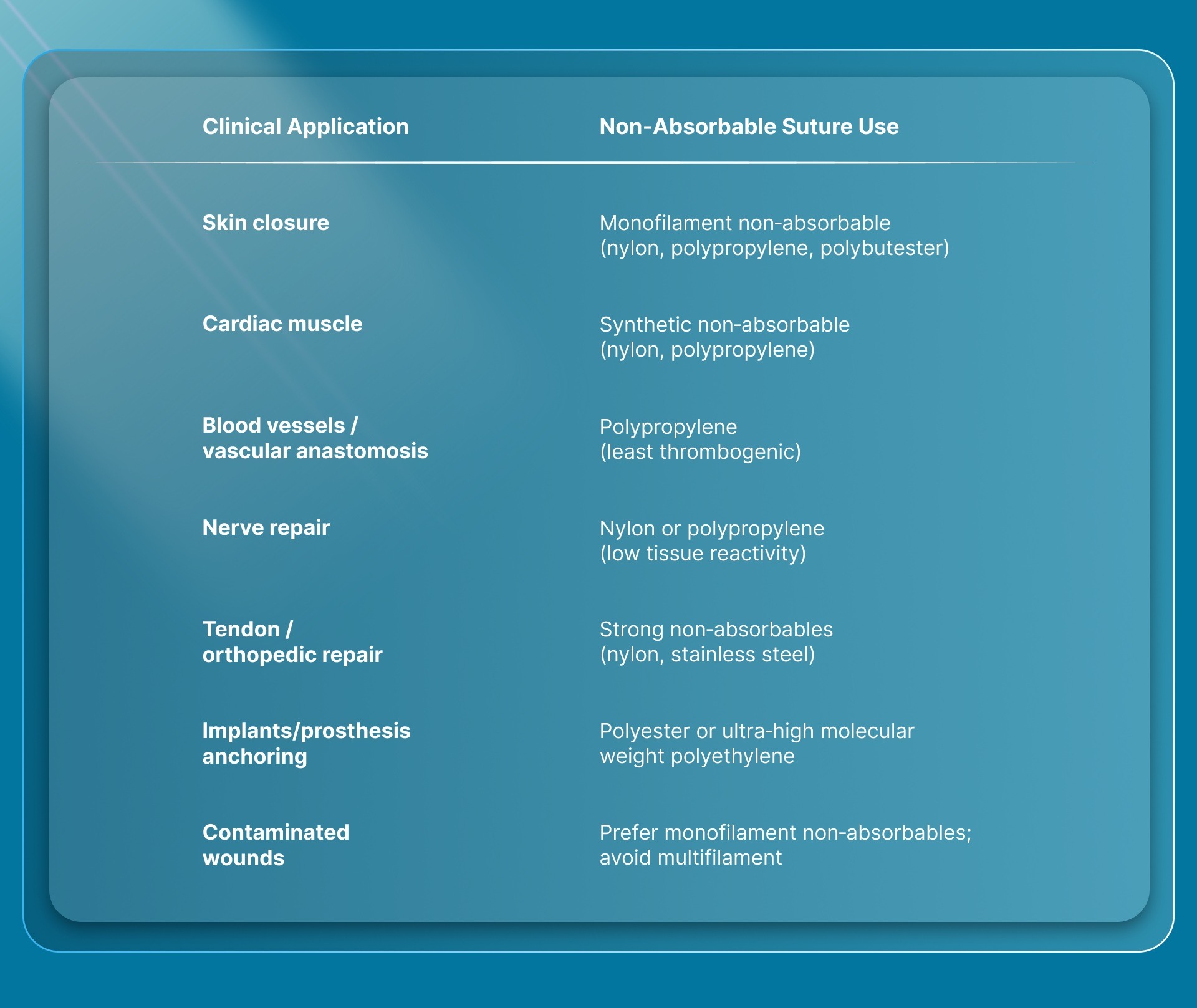
1. Skin and Superficial Closure: Used to close cutaneous incisions and traumatic lacerations because they provide secure wound edge approximation and can be removed once healing is sufficient.
2. Highly Dynamic or Stressed Areas: Employed in regions exposed to tension and movement (e.g., abdominal wall, hernia repairs) where prolonged support improves healing and reduces dehiscence.
3. Vascular and Cardiac Surgery: Monofilament non‑absorbable sutures (e.g., polypropylene) are preferred for vascular anastomoses and vessel repairs because of their strength and minimal thrombogenicity.
4. Nerve and Soft Tissue Repair: Non‑absorbable sutures with low tissue reactivity are chosen when precise alignment and long‑term support are crucial, such as in nerve repair.
5. Implant and Prosthetic Fixation: Strong synthetic non‑absorbables (e.g., PET or ultra‑high molecular weight polyethylene) may be used to anchor implants or in procedures requiring permanent mechanical support (e.g., joint stabilization).
6. Orthopedic and Deep Tissue Repair: In orthopedic surgeries and deep fascia closures, braided and high‑strength non‑absorbable sutures are used where prolonged integrity under load is needed.
Non‑Absorbable Sutures: Removal Windows by Body Area
Non‑absorbable sutures do not dissolve in the body and must be removed when used for superficial skin closure once the wound has gained sufficient strength. Skin healing varies by body area, and surgeons time suture removal to balance wound support with minimizing scarring.
Non‑absorbable sutures are commonly used for external skin closure because they provide durable support and are easier to remove than many absorbable alternatives.
When Are Non‑Absorbable Sutures Removed?
Typical removal times for non‑absorbable skin sutures are:
- Face and neck: removed early (about 4–6 days) due to rapid healing and cosmetic priority.
- Other body areas: generally removed between 8–14 days, allowing adequate tissue strength before suture removal.
Note: Exact timing depends on location, tension on the wound, and healing response; for example, higher‑tension or slower‑healing areas may warrant longer support before removal.
Internal vs External Use
- External (skin): sutures are removed once the wound is stable and healed enough to maintain closure without support.
- Internal use: non‑absorbable sutures placed deep (e.g., in vascular or muscle repairs) are typically left permanently because they are designed to be biocompatible and to provide long‑term strength without removal.
Key point: Non‑absorbable sutures used on the skin are removed at specific intervals based on healing rates, while those used internally usually remain in place permanently to support tissues over time.
SubQ It!: A Smarter Alternative to Non-Absorbable Sutures

While non-absorbable sutures are widely used for durable wound closure, they often require removal and can impact cosmetic outcomes. SubQ It! offers a bioabsorbable subcuticular alternative that delivers fast closure without removal, bridging the gap between sutures and staples.
Key Features & Benefits
- Bioabsorbable, Subcuticular Closure: fasteners are placed beneath the skin and naturally absorbed during healing—no removal visit.
- Faster Than Sutures: Deploys each fastener in ~7 seconds, up to 7× faster than manual suturing, reducing OR time.
- Two Time-Saving Models
- SubQ It 10: 10 fasteners, up to 10 cm (small/laparoscopic incisions)
- SubQ It 25: 25 fasteners, up to 25 cm (longer incisions)
- Minimized Scarring: Subcuticular placement avoids external skin puncture, reducing visible scarring vs metal staples.
- No Follow-Up for Removal: Eliminates staple removal visits, improving patient experience and workflow efficiency.
- Broad Surgical Use: Suitable for abdominal, orthopedic, and minimally invasive procedures.
- Cost Consideration: ~$60–$100 per use; time savings can offset cost in high-volume settings
Final Thoughts
Non-absorbable sutures remain essential where sustained tensile strength is required, particularly in high-tension and slow-healing tissues. Their reliability makes them a standard choice across vascular, orthopedic, and fascial closures.
At the same time, outcomes depend on more than durability. Material selection and filament structure directly influence infection risk, tissue response, and intraoperative efficiency, making context-driven choice critical.
For more efficient and consistent closure in skin and superficial tissues, bioabsorbable subcuticular systems like SubQ It! offer a practical shift. They eliminate removal steps, reduce visible scarring, and streamline workflow while maintaining reliable wound support.
Maximize closure efficiency by choosing solutions that align with both tissue demands and real-world surgical workflows. Reach out to explore how SubQ It! can support your practice.
FAQs
1. What are non-absorbable sutures, and how do they work?
Non-absorbable sutures are materials that resist degradation in the body and maintain tensile strength over time, providing long-term tissue support instead of being absorbed during healing.
2. When should non-absorbable sutures be used instead of absorbable ones?
They are preferred in high-tension or slow-healing tissues such as fascia, tendons, and vascular repairs, where prolonged mechanical support is required.
3. What are the main types of non-absorbable suture materials?
Common types include nylon, polypropylene, polyester, silk, and stainless steel, each offering different levels of strength, flexibility, and tissue reactivity.
4. What is the difference between monofilament and multifilament non-absorbable sutures?
Monofilament sutures are single-stranded with lower infection risk, while multifilament sutures are braided for better handling and knot security but higher capillarity.
5. Do non-absorbable sutures always need to be removed?
Surface (skin) sutures typically require removal after healing, while those placed internally are often left permanently to provide ongoing support.
6. What are the risks or disadvantages of non-absorbable sutures?
Key limitations include the need for removal, potential infection (especially with braided sutures), and tissue reaction depending on the material.