Introduction
Skin closure plays a critical role in operative efficiency, healing, and follow-up. In high-volume settings, even small differences in technique can affect turnover and overall outcomes.
The closure method also influences clinical results. Studies show that, in renal transplant patients, infection rates were 24% with staples versus 8% with sutures. This shows the importance of selecting the right approach for each case.
Metal staples are commonly used to standardize and speed closure, especially in longer procedures, but they require removal and can affect cosmetic outcomes.
In this blog, you will learn when surgeons use surgical staples, where they are most effective, how they are placed, and the best practices that guide their safe use.
Key Takeaways:
- Surgical staples are selected based on incision type, tissue characteristics, and procedural efficiency.
- Proper technique, including correct device selection, perpendicular placement, and consistent spacing, prevents complications.
- Staples are most effective for linear, well-approximated wounds, particularly in longer incisions, where closure time affects the overall operative workflow.
- Internal staplers are widely used in gastrointestinal, thoracic, and bariatric procedures for faster, consistent tissue handling.
- Removal timing varies by anatomical location and patient factors, making post-operative planning an important part of staple-based wound closure.
When Should Surgeons Use Surgical Staples?
Surgical staples are primarily used when closure speed, consistency, and procedural efficiency are prioritized over fine cosmetic outcomes.
In practice, surgeons select staples based on incision type, tissue characteristics, and operative workflow rather than a single factor such as tension or location.
The following scenarios outline where stapling is most appropriate in clinical use.
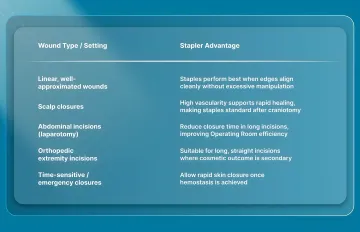
1. Ideal Stapler Applications:
Surgical staples are most effective for wound types in which rapid closure and consistent edge approximation can be achieved without complex tissue handling.
Their use is typically determined by incision characteristics, tissue quality, and the need to maintain operating-room efficiency.
Beyond general use cases, comparative data provide additional perspective on outcomes associated with staple closure.
Real Case Study:
In a multicentre randomized controlled trial of 300 patients undergoing elective vascular surgery, researchers compared skin closure using metal staples versus intradermal sutures.
The study focused on surgical site infection rates and incision-related complications following groin incisions.
- Results showed that 15.8% of patients in the staple group developed surgical site infections, compared to 10.1% in the intradermal suture group.
In addition to infection rates, other complications were also evaluated:
- 21.1% of patients in the staple group experienced seroma or lymphatic leak, compared to 12.8% in the suture group
- Overall, incision-related complications were reported in 19.7% of staple closures, compared with 13.5% with sutures.
These findings reinforce that while staples offer speed and consistency, the selection of closure methods should be guided by procedural context, tissue characteristics, and postoperative considerations.
2. Internal Stapler Applications
Surgical staplers are not limited to skin closure. In many procedures, they are essential for tissue division, resection, and reconstruction, where speed and consistency directly impact operative outcomes.
The following are the primary internal applications where stapling devices are routinely used.
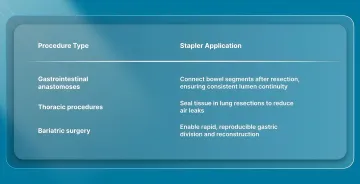
Internal staplers are designed to simultaneously cut and staple tissue, creating secure, uniform staple lines while significantly reducing operative time compared to hand-sewn techniques.
While staplers serve many procedural needs, certain wound types require alternative closure approaches.
When Surgical Staples Are Less Appropriate?
Staples are not suitable for every wound. Selection depends on tissue characteristics, cosmetic requirements, and the ability to achieve stable approximation without excessive tension.
Avoid or reconsider staple use in the following scenarios:
- Cosmetically sensitive areas: Face, neck, and hands, where subcuticular closure provides superior aesthetic outcomes
- Irregular or jagged wounds: Where uniform edge approximation cannot be achieved
- High-tension wounds without layered closure: Requires deep sutures to offload tension before skin closure
- Fragile or thin skin: Increased risk of tearing or poor staple hold
Even when staples appear technically appropriate, broader clinical factors must still be evaluated.
Clinical Considerations:
In addition to wound characteristics, patient-specific factors influence closure decisions and outcomes.
- Compromised perfusion: Poor blood supply increases the risk of delayed healing and wound complications
- Contaminated or infected wounds: May require delayed or staged closure rather than immediate stapling.
- General wound healing risk factors: Age, medications, and systemic conditions may affect closure method selection
Knowing when staples are appropriate also requires proper preparation before application.
A Checklist of Everything You Need Before Using Surgical Staples
Effective stapling depends on selecting the correct device, properly preparing the tissue, and using a controlled deployment technique.
Before placing staples, the following requirements should be met:
Required Equipment:
- Appropriate stapling device: Skin staplers for external closure; linear or circular staplers for internal tissue division and anastomosis. In procedures involving longer incisions, SubQ It! SU-25 may be used to achieve consistent dermal approximation without the need for external staple placement.
- Correct staple cartridge selection: Must match tissue thickness and type, as improper selection increases the risk of incomplete staple formation or tissue injury
- Prepared wound bed: Hemostasis achieved, nonviable tissue debrided, and wound adequately irrigated to support stable closure
- Tissue handling instruments: Forceps or skin hooks used to evert and align wound edges for accurate staple placement
Operator Requirements:
Stapling devices standardize closure, but their safety and effectiveness depend heavily on correct intraoperative use.
- Training in stapler use and tissue handling: Improper use is a leading contributor to device-related complications, including staple misfire, bleeding, and incomplete closure
- Adequate visualization and access: Clear exposure of the operative field is necessary to ensure precise placement and safe deployment.
- Verification of surrounding structures: Particularly in internal stapling, adjacent vessels, nerves, and organs must be protected before firing to avoid serious injury
A thorough pre-use check supports the next stage: placing the staples consistently and with care.
5 Steps to Take for Placing Surgical Staples Effectively
Surgical stapling requires a controlled technique to ensure proper staple formation and consistent wound approximation. Errors in positioning, deployment, or spacing can result in malformed staples, tissue injury, or wound dehiscence.
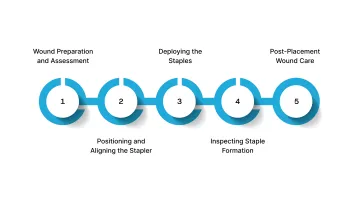
The following sequence outlines the key steps for safe and effective staple placement:
1. Wound Preparation and Assessment
Before placing staples, ensure the wound is appropriately prepared:
- Achieve hemostasis: Active bleeding interferes with staple formation and increases hematoma risk
- Assess wound edges: Confirm viable tissue and adequate edge approximation without excessive tension
- Debride nonviable tissue: Remove compromised tissue that may impair healing
- Irrigate thoroughly: Cleanse the wound according to surgical protocol
2. Positioning and Aligning the Stapler
Proper positioning determines staple formation and the quality of closure.
- Evert wound edges using forceps or skin hooks to achieve dermal-to-dermal contact
- Position the stapler perpendicular to the wound line, centered over the incision
- Maintain consistent spacing (approximately 0.5–1 cm) to ensure uniform tension and preserve tissue perfusion
3. Deploying the Staples
With the stapler properly positioned:
- Apply gentle pressure to approximate wound edges
- Activate the stapler in a single, controlled motion
- Maintain perpendicular alignment during deployment to avoid uneven staple formation
- Ensure full deployment before releasing the device
Incomplete or misaligned deployment can result in malformed staples, which should be removed and replaced immediately.
4. Inspecting Staple Formation
Each staple should be evaluated immediately after placement:
- Proper formation: Staples should form a uniform “B-shape” with even penetration
- Wound alignment: Edges should be approximated without gaps, overlap, or excessive tension
- Identify malformations: Incomplete penetration, asymmetry, or over-compression
Any improperly formed staple should be removed and replaced to maintain the integrity of the closure.
5. Post-Placement Wound Care
Follow these steps for post-placement wound care:
- Apply dressing based on wound type and expected drainage
- Document staple count and wound characteristics
- Provide clear instructions for care and removal timing based on anatomical location
Following the correct placement steps creates consistency, but long-term results depend on broader best practices.
Best Practices for Using Surgical Staples Effectively
Effective wound closure requires balancing speed, reliability, and clinical outcomes across different surgical contexts. Staple use should be guided by tissue characteristics, procedural demands, and post-operative management considerations.
The following factors help determine the most appropriate closure approach in practice:
1. Key Closure Considerations:
When selecting a closure method, surgical teams should evaluate:
- Tissue thickness and tension: Staple selection and spacing must align with tissue characteristics to ensure proper formation and avoid excessive compression
- Patient healing capacity: Factors such as perfusion, comorbidities, and medication use influence closure choice and complication risk
- Cosmetic outcome requirements: Subcuticular techniques are generally preferred in cosmetically sensitive areas
- Operating room efficiency: Staples reduce closure time compared to sutures, particularly in longer incisions
- Post-operative care requirements: External staples require removal, adding a follow-up step to the care pathway
2. Bioabsorbable Subcuticular Approach
Bioabsorbable subcuticular closure systems provide an alternative to external staples by placing fasteners beneath the skin surface.
- No removal required: Eliminates the need for a follow-up visit for staple removal
- Subcuticular placement: Avoids external skin puncture, reducing visible surface marks
- Comparable procedural efficiency: Designed to maintain closure speed while improving workflow consistency
These systems are particularly relevant in procedures where both efficiency and cosmetic outcome are priorities.
Final Thoughts
Skin closure decisions extend beyond the operating room, influencing how consistently wounds heal, how follow-up is managed, and how predictable outcomes remain across different surgical settings.
As procedural demands increase, surgeons are placing greater emphasis on closure methods that reduce variability without adding complexity to workflow.
In this context, systems like SubQ It! SU-25, designed for incisions up to 25 cm, offer a subcuticular, device-assisted approach for longer procedures. It helps reduce closure time by approximately 25 minutes per case while eliminating the need for staple removal.
Get in touch with us to explore how SubQ It! SU-25 supports efficient closure and consistent outcomes in longer incisions.
FAQs
1. How long do surgical staples usually stay in?
External skin staples are typically removed within 7–14 days, depending on the anatomical location and wound characteristics. Timing may be extended based on patient factors, including wound tension, healing capacity, and comorbidities.
2. Why do surgeons use staples instead of stitches?
Staples are used primarily for speed and consistency of closure, particularly in longer or time-sensitive procedures. They allow rapid approximation of wound edges and reduce operative time, while sutures remain preferred in areas requiring precise cosmetic outcomes.
3. Is it painful to have surgical staples removed?
Staple removal causes brief discomfort, often known as a pulling or pinching sensation, and is generally well tolerated. In most cases, removal is performed without anesthesia, although local measures may be used in sensitive patients.
4. What are surgical staples made of?
Most surgical staples are made from titanium or stainless steel, both of which provide strength and biocompatibility. Bioabsorbable alternatives use polymer-based materials that gradually degrade in the body, eliminating the need for removal.
5. Can I have an MRI with surgical staples?
Titanium staples are considered MRI-safe and produce minimal imaging artifact. Stainless steel staples are generally safe but may cause more distortion. Bioabsorbable polymer-based systems contain no metal and do not interfere with imaging.
6. Can you shower with staples in the abdomen?
Titanium staples are considered MRI-safe and produce minimal imaging artifact. Stainless steel staples are generally safe but may cause more distortion. Bioabsorbable polymer-based systems contain no metal and do not interfere with imaging.