Absorbable sutures are a routine part of wound closure, but the choice of material still carries clinical weight.
Reports show that approximately 72% of U.S. hospitals use advanced absorbable sutures for internal closures, reflecting how widely surgeons rely on temporary internal support.
The decision is rarely about absorption alone. Tissue depth, wound tension, healing time, and cosmetic priority all shape which material is appropriate.
In this blog, you’ll explore how surgeons evaluate absorbable sutures in 2026, including material properties, strength retention, tissue response, and procedural considerations.
Key Takeaways:
- Absorbable sutures provide temporary wound support and gradually break down in the body, so removal is typically not required.
- Suture choice depends on tissue depth, wound tension, healing time, and the level of support required during recovery.
- Synthetic absorbable sutures usually offer more predictable absorption, while natural sutures may create a stronger tissue response.
- Strength retention matters more than total absorption time because sutures can lose functional support before they are fully absorbed.
- Monofilament and braided absorbable sutures differ in handling, knot security, tissue drag, and suitability for different surgical fields.
What Are Absorbable Sutures?
Absorbable sutures are sterile surgical materials used to hold tissue together during healing. They gradually lose tensile strength and are broken down by the body, so they typically do not require removal.
Surgeons use absorbable sutures when temporary wound support is enough, such as internal tissue closure, mucosal closure, or subcuticular skin closure. The material must match the rate of tissue healing and the duration of support needed.
Defining what absorbable sutures are also provides a clear foundation for understanding their core characteristics.
4 Core Characteristics of Absorbable Sutures
Absorbable sutures differ in how they break down, how long they hold strength, and how much tissue response they create. These factors determine whether the material can support the wound long enough without remaining in the tissue longer than needed.
Below are the core characteristics of absorbable sutures.
1. Absorption Mechanism and Timeline
Synthetic absorbable sutures usually degrade through hydrolysis, while natural absorbable sutures degrade through enzymatic breakdown.
Synthetic materials generally offer more predictable absorption, while natural materials can create a stronger tissue response.
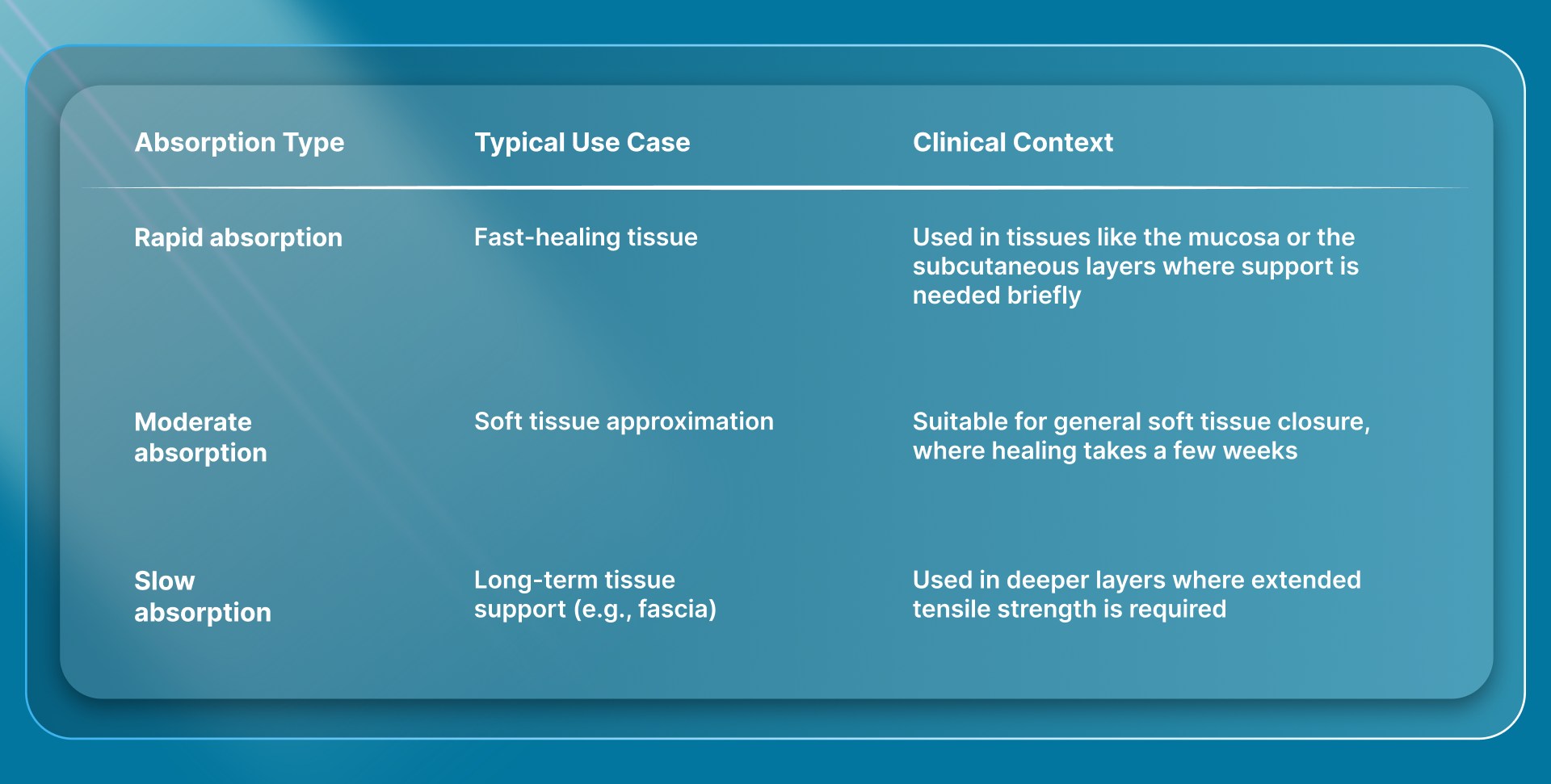
Absorption timing varies by material and product type:
2. Tensile Strength Profile
Tensile strength determines how long the suture can support tissue during healing. A suture may lose functional strength before it is fully absorbed, so surgeons usually assess both strength retention and total absorption time.
For example, fascia typically needs longer support than mucosa or superficial tissue. Slower-absorbing materials such as polydioxanone are commonly considered when extended wound support is needed.
3. Tissue Reactivity
Tissue reactivity refers to the local inflammatory response caused by the suture material. Synthetic absorbable sutures generally cause less tissue reaction than natural gut sutures because they break down through hydrolysis instead of enzymatic digestion.
This matters most in areas where inflammation or foreign-body response may influence healing response and cosmetic outcomes.
4. Handling and Knot Security
Handling affects how easily the suture passes through tissue, ties securely, and stays in place during closure.
- Braided sutures: Better handling and knot security
- Monofilament sutures: Lower tissue drag but higher memory, requiring more careful knot placement
For longer incisions, handling is not only about how the material ties. It also affects how consistently and efficiently the closure can be completed.
This is where subcutaneous bioabsorbable closure systems, such as SubQ It! SU-25 becomes relevant, especially for surgeons seeking to reduce manual placement and knot-tying time without using external metal staples.
Once you understand the core characteristics, it becomes easier to examine the different types and structural variations of absorbable sutures.
4 Key Types and Structures of Absorbable Sutures
Absorbable sutures are usually classified as natural or synthetic. For surgeons, the main difference is how predictably they lose strength, how they handle in tissue, and how much tissue reaction they may create.
Below are the four types of absorbable sutures.
1. Natural Absorbable Sutures
Natural absorbable sutures are commonly made from purified collagen and break down through enzymatic degradation.
They are less predictable than synthetic absorbable sutures and are generally associated with higher tissue reactivity, so they are usually selected for specific short-term closure needs.
- Plain gut: Generally provides short-term support and is often used for fast-healing tissue. It maintains tensile strength for about 7 to 10 days and is absorbed over roughly 70 days.
- Chromic gut: Treated with chromium salts to slow absorption and extend support compared with plain gut. It commonly maintains tensile strength for about 21-28 days and is absorbed over roughly 90 days.
2. Synthetic Absorbable Sutures
Synthetic absorbable sutures degrade primarily by hydrolysis, making their absorption more predictable. They are commonly used for soft tissue approximation when you need a clearer strength-retention profile.
- Polyglactin 910, Vicryl: A braided synthetic absorbable suture. It retains about 75% tensile strength at 2 weeks and 50% at 3 weeks, with absorption usually completed in 56 to 70 days.
- Poliglecaprone 25, Monocryl: A monofilament synthetic absorbable suture used for soft tissue approximation and ligation. Complete absorption is reported between 91 and 120 days, with slight or minimal tissue reaction in published material data.
- Polyglycolic acid, Dexon: A braided synthetic absorbable suture with a profile similar to polyglactin 910. It is used where absorbable support, handling, and knot security are clinically relevant.
3. Slowly Absorbable Synthetic Sutures
Slowly absorbable sutures are used when tissue needs support for a longer healing period. These materials are especially relevant in deeper closures where early loss of tensile strength could compromise wound support.
- Polydioxanone, PDS II: A monofilament synthetic absorbable suture used when extended wound support is needed. Ethicon product data lists absorption at 180 to 210 days, with strength retention varying by suture size.
- Polyglyconate, Maxon: Another monofilament, slowly absorbable synthetic suture used for longer-support closures. Keep this mention brief unless the blog later compares extended-support sutures in detail.
4. Monofilament vs Multifilament Absorbable Sutures
Suture structure affects handling, knot security, tissue drag, and infection risk. This should be treated as a selection factor, not repeated across every suture type.
- Monofilament absorbable sutures: Like Monocryl and PDS, which have a single smooth strand. They usually pass through tissue with less drag, but they may have more memory and require a careful knot technique.
- Multifilament absorbable sutures: Like Vicryl and Dexon, which are braided. They usually handle well and provide stronger knot security, but the braided structure may be less ideal in contaminated fields.
A clear understanding of the different types and structures also provides useful context for surgeons' selection of absorbable sutures for specific procedures.
How Surgeons Select Absorbable Sutures for Different Procedures?
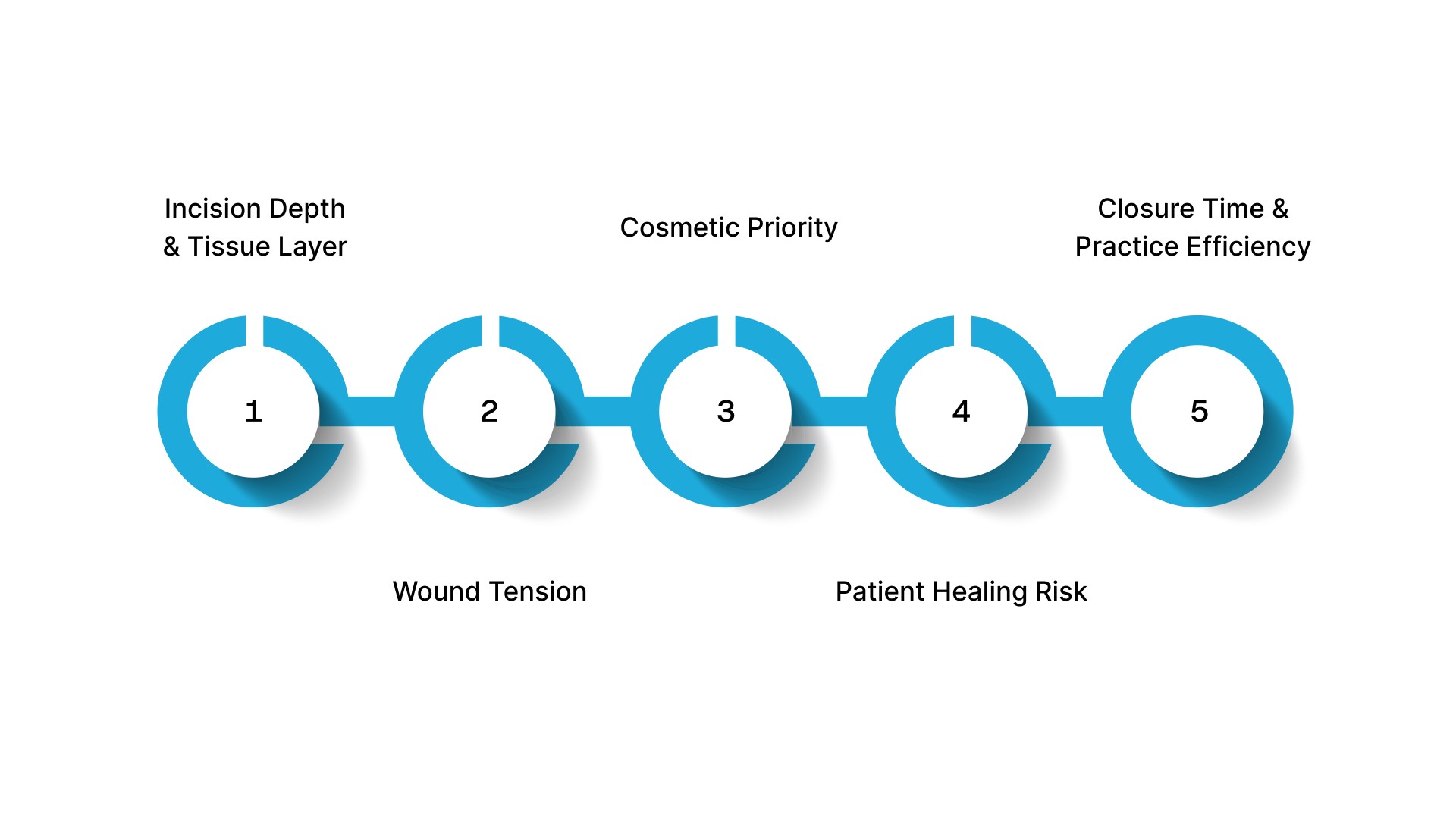
Surgeons select absorbable sutures by matching the closure material to the procedure, tissue layer, and healing demands. The choice affects wound support, cosmetic outcome, patient experience, and follow-up requirements.
Here’s how surgeons select absorbable sutures for different procedures:
1. Incision Depth and Tissue Layer
Different tissue layers need different levels of wound support. A superficial closure may only require short-term support, whereas a fascial or deeper soft-tissue closure may require longer-term support.
- Superficial closures usually need temporary support during early healing.
- Deeper tissue layers need materials that hold strength longer.
- The selected suture must support the tissue long enough to avoid early separation.
- Strength retention matters more than total absorption time during active healing.
2. Wound Tension
Wound tension changes how much support the closure needs. Areas under movement, pressure, or pull usually require stronger, longer-lasting support.
- High-tension areas include abdominal closures, joints, and mobile tissue planes.
- Low-tension areas may use materials that lose strength sooner.
- Closure choice should match the mechanical stress on the wound.
- Poor material selection can increase the risk of wound edge separation.
3. Cosmetic Priority
Cosmetic outcome matters in plastic surgery, especially at visible incision sites. Surgeons usually focus on clean tissue approximation, controlled tension, and minimal tissue trauma.
- Visible incision sites need careful closure planning.
- Subcuticular closure is often used when scar appearance matters.
- Excessive tissue reaction can affect the final scar.
- Closure speed should not come at the cost of precision in cosmetic cases.
4. Patient Healing Risk
Patient factors can change how long a wound needs support. Healing may be slower in patients with metabolic, vascular, nutritional, or tissue-quality concerns.
- Diabetes, obesity, smoking history, and poor nutrition can slow healing.
- Older patients or patients with fragile tissue may need gentler handling.
- Steroid use or immunosuppression can affect wound strength.
- Higher-risk patients may need longer support or a more cautious closure plan.
5. Closure Time and Practice Efficiency
Closure choice also affects case flow, especially for clinic-owning surgeons. Absorbable sutures reduce the need for removal visits, but manual placement and knot tying still take time during the procedure.
- Longer incisions create greater pressure on closure time.
- High-volume practices need closure methods that support efficient use of rooms.
- Reducing closure time can improve scheduling capacity.
- The best closure choice balances cosmetic outcome, wound support, and procedural efficiency.
Final Thoughts
Absorbable suture selection affects more than tissue support. It also shapes consistency in closure, follow-up planning, and efficiency across longer procedures.
As surgeons seek to preserve cosmetic outcomes while reducing manual closure time, closure systems are being evaluated beyond material selection alone.
In this context, SubQ It! SU-25 uses 25 bioabsorbable staples to close incisions up to 25 cm, making it relevant for longer incisions in open surgeries and plastic surgery procedures.
By saving approximately 25 minutes per case, it also offers a clear efficiency and economic advantage for private clinic owners.
Contact us today to learn how SubQ It! SU-25 can fit into your current closure workflow.
FAQs
1. Which types of sutures are absorbable?
Absorbable sutures include plain gut, chromic gut, Vicryl, Dexon, PDS, Monocryl, and Maxon. They break down in the body over time through enzymatic degradation or hydrolysis, so removal is usually not required.
2. What materials are absorbable sutures made of?
Natural absorbable sutures are commonly made from purified collagen. Synthetic absorbable sutures are made from polymers such as polyglycolic acid, polydioxanone, polyglactin 910, and poliglecaprone 25.
3. How long do absorbable sutures take to absorb?
Absorption time depends on the material. Some absorbable sutures lose strength within days or weeks, while slower-absorbing materials such as PDS may remain for several months. Surgeons usually focus on strength retention first, because a suture can lose functional support before it is fully absorbed.
4. How do surgeons know if sutures are absorbable?
Absorbable sutures are identified on the product label and packaging. In practice, surgeons select the material based on tissue type, healing time, wound tension, and whether suture removal would add unnecessary follow-up.
5. When do surgeons use Monocryl vs Vicryl?
Surgeons often use Monocryl for subcuticular or soft-tissue closure, where a smooth monofilament structure is preferred. Vicryl is commonly used for soft-tissue approximation when braided handling and knot security are desired. The choice depends on tissue layer, tension, infection risk, and the desired absorption profile.
6. Can patients react to absorbable sutures?
Yes, but clinically significant reactions are uncommon. Natural gut sutures generally create more tissue reaction than synthetic absorbable sutures, while synthetic materials tend to have a more predictable response.
7. What are the benefits of using absorbable sutures?
Absorbable sutures provide temporary wound support and gradually break down in the body, so removal is usually not required. They are commonly used for internal closures and can reduce the need for follow-up visits.
8. What are the downsides of using absorbable sutures?
Absorbable sutures lose strength over time, so they may not be suitable for long-term support. Some materials may elicit a greater tissue reaction than others, and improper selection can lead to early loss of support.
9. How do patients care for their stitches?
Post-operative care depends on the procedure and location of the wound. Patients are usually advised to keep the area clean, follow dressing instructions, and avoid excessive stress on the wound. Specific instructions should always come from the treating surgeon.