The way surgical wounds are closed impacts everything from recovery speed to cosmetic results.
In the United States, surgical site infections remain a significant concern, affecting roughly 110,800 inpatient cases annually, with estimates ranging up to 500,000.
Metal staples offer rapid closure but require removal, whereas manual sutures provide precise approximation in cosmetically sensitive areas, though they take longer to place.
Absorbable closure devices, on the other hand, support healing. They naturally degrade over time, providing temporary tissue support.
In this blog, you’ll explore why surgeons in 2026 are adopting absorbable wound closure devices, including their advantages across surgical specialties, the types available, and practical guidance for selecting the most effective system.
Key Takeaways:
- Absorbable wound closure devices offer temporary tissue support during healing and typically do not require removal, simplifying postoperative care.
- Device selection depends on wound characteristics, tissue type, tension, and required support duration.
- Barbed sutures, traditional sutures, subcuticular staplers, and tissue adhesives each differ in mechanism, handling, and clinical use.
- The choice of closure method influences surgical workflow, follow-up requirements, and overall care processes.
- Effective outcomes rely on matching the device and technique to the clinical scenario.
What Are Absorbable Wound Closure Devices?
Absorbable wound closure devices are made from bioabsorbable materials that the body gradually breaks down, providing temporary support as tissues heal.
These devices are used across a wide range of surgical specialties, depending on the type of tissue and clinical requirement, including:
- General surgery: Abdominal and laparoscopic procedures
- Plastic surgery: Closures where cosmetic outcome is important
- Gynecology: Procedures such as cesarean sections and hysterectomies
- Orthopedics: Fracture fixation, joint replacement, and soft tissue repair involving ligaments and tendons
There’s recent clinical evidence that highlights the effectiveness of absorbable wound closure devices.
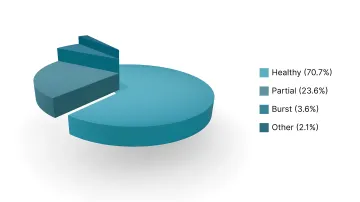
Real Case Study:
A 2025 observational study of 140 emergency laparotomy patients using barbed delayed absorbable polydioxanone (PDS) sutures reported that 70.7 % had healthy suture lines by postoperative day 8.
Along with that, 23.6 % required partial opening of skin sutures, and the incidence of burst abdomen was only 3.6 % in the PDS group.
This study shows that while minor wound management interventions may still be required, the low incidence of major complications supports the use of absorbable wound closure devices in maintaining fascial closure strength.
Knowing the purpose and function of these devices provides insight into their importance during surgery.
Why are Surgeons in the US Relying on Absorbable Wound Closure Devices?
The choice of wound closure method affects both surgical workflow and post-operative management in 2026. Surgeons prefer absorbable wound closure devices for the following reasons:
1. Helps Improve the Patient Experience and Recovery
These wound closure devices remove the need for a separate staple removal procedure, simplifying post-operative care.
- Subcuticular techniques avoid placing material across the external skin surface.
- Reduce visible surface marks compared to percutaneous closure methods
2. Supports Surgical Efficiency and Workflow
Absorbable wound closure devices can influence workflow depending on the device type and application method. Some are designed for faster deployment, while others prioritize precision and tissue support.
- Reduce the workload associated with suture or staple extraction
- Can support a more simplified workflow in high-volume surgical settings
3. Promotes Consistent Clinical Outcomes
Absorbable wound closure devices influence the consistency with which outcomes are achieved across surgical teams and clinical settings.
- Help reduce technique-dependent variability in closure outcomes across surgical teams.
- Align material degradation with tissue-healing timelines to avoid prolonged exposure to a foreign body.
Seeing how these devices affect surgical outcomes makes it clear why each type matters.
4 Types of Absorbable Wound Closure Devices Used in Surgery
Absorbable wound closure devices include multiple categories with different mechanisms, materials, and clinical applications. Below are the different types of wound closure devices.
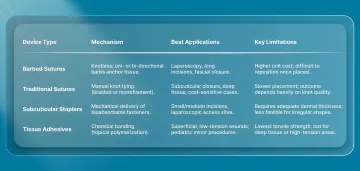
1. Absorbable Barbed Sutures
Absorbable barbed sutures are knotless sutures with uni-directional or bi-directional barbs along the filament. These barbs engage tissue as the suture is advanced, reducing the need for knot tying.
Examples include V-Loc, Quill, and Stratafix.
| Best Applications | Limitations |
|---|---|
| Laparoscopic procedures where knot tying is technically challenging | Higher cost compared to conventional sutures |
| Long incisions that require continuous tension distribution | Require familiarity with technique and tension control |
| Fascial closure and soft tissue approximation | Repositioning after placement may be limited due to tissue anchoring |
| Situations requiring uniform wound edge alignment | Improper use may increase tissue resistance or localized trauma |
2. Traditional Absorbable Sutures
Traditional absorbable sutures are polymer-based sutures that require manual knot tying for fixation.
Common materials include polyglactin (Vicryl), poliglecaprone (Monocryl), and polydioxanone (PDS). They are available in braided and monofilament forms.
| Best Applications | Limitations |
|---|---|
| Subcuticular closure in cosmetically sensitive areas | Slower to place due to knot tying |
| Deep tissue approximation that requires sustained support | Outcomes depend on surgical technique and knot quality |
| Pediatric and general surgical use | Knot-related complications may occur in some cases |
| Situations where cost considerations are relevant | Greater technical demand in minimally invasive procedures |
3. Absorbable Subcuticular Stapler Systems
Absorbable subcuticular stapler systems are mechanical devices that deploy bioabsorbable fasteners within the dermal layer beneath the skin surface.
Examples of this category include systems such as SubQ It! SU-25, which can close incisions up to 25 cm. This makes it suitable for both small and large incisions across a wide range of surgical procedures.
| Best Applications | Limitations |
|---|---|
| Small to medium surgical incisions | Higher device cost compared to sutures |
| Laparoscopic access sites | Limited flexibility for complex or irregular wound shapes |
| Situations where subcuticular closure is preferred | Device size and fastener count may limit use in longer incisions |
| Procedures where both efficiency and cosmetic outcome are considerations | Require adequate dermal tissue for effective placement |
4. Absorbable Tissue Adhesives and Sealants
Absorbable tissue adhesives are topical agents that bond skin edges together by polymerizing on contact with tissue moisture. Common formulations include cyanoacrylate-based adhesives.
| Best Applications | Limitations |
|---|---|
| Superficial, low-tension wounds | Not suitable for high-tension wounds |
| Pediatric or minor procedures | Lower tensile strength than sutures or mechanical closure systems |
| Adjunct use over deeper closure methods | Not used for deep tissue approximation |
| Outpatient settings that require a quick application | Performance depends on proper wound edge alignment |
Once you understand the different types of absorbable wound closure devices, it helps highlight common pitfalls to avoid when selecting the right one.
Avoid These Pitfalls When Choosing Absorbable Wound Closure Devices

Inappropriate selection of absorbable wound closure devices can affect surgical workflow, healing outcomes, and overall resource use. These issues typically arise from mismatches between device properties and the wound's clinical requirements.
1. Overengineering the Solution
Choosing a more complex or higher-cost absorbable wound closure device when a simpler option would be sufficient can add unnecessary cost and handling complexity without improving outcomes.
- More advanced devices are not always required for low-tension or straightforward closures.
- Simpler sutures or closure methods may provide comparable results in appropriate cases.
- Selection should be based on wound requirements rather than perceived technological advantage.
2. Absorption Timeline Mismatch
Using a device with an absorption profile that does not meet tissue-healing requirements can compromise wound support.
- Rapidly absorbing sutures are designed for short-term support in superficial tissues.
- These materials lose tensile strength relatively early after placement
- They are not suitable for closures requiring prolonged mechanical support, such as fascia
3. Ignoring Total Cost of Care Considerations
Focusing only on the upfront cost of an absorbable wound closure device can overlook broader procedural and post-operative factors.
- Device choice can influence operative workflow and closure time
- Some methods may reduce or eliminate the need for removal procedures
- Overall impact depends on total care cost, not acquisition cost alone
4. Selection Based on Familiarity Instead of Clinical Fit
Relying on familiar techniques without evaluating alternatives may limit optimization of outcomes.
- Surgeons may default to techniques they are most experienced with
- Different wound types require different closure approaches
- Device selection should be based on tissue characteristics, wound mechanics, and procedural needs
Understanding the common challenges in selecting absorbable wound closure devices helps ensure the right choice for each procedure.
4 Key Factors in Selecting the Right Absorbable Wound Closure Device
Selecting an absorbable wound closure device becomes complex because materials differ in strength retention, absorption rate, and handling characteristics. Without a structured approach, mismatched selection can lead to early loss of support or unnecessary tissue reaction.
Here’s how to select the right device:
1. Tissue Biomechanics and Wound Parameters
Start by assessing what you are closing, as tissue type and mechanical demands determine the required performance.
- Tissue depth determines the required support duration: Superficial tissues, such as skin, heal quickly and require short-term support, while fascia and deeper layers require prolonged tensile strength to maintain closure during healing.
- Wound tension dictates material strength: High-tension areas require materials that retain strength longer, whereas low-tension closures allow faster-absorbing options.
- Wound geometry influences closure technique: Linear wounds are simple, while irregular or complex wounds may require more adaptable or layered closure approaches.
2. Strength Retention and Absorption Kinetics
Once tissue requirements are clear, match the device’s strength profile to the healing timeline.
- Strength retention must align with tissue healing: Closure materials should maintain adequate tensile strength until the tissue regains sufficient intrinsic strength.
- Rapidly absorbing materials suit fast-healing tissues: These are appropriate for superficial layers where prolonged support is unnecessary.
3. Procedural Context and Intraoperative Considerations
Procedure type and access conditions directly influence device selection and handling.
- Procedure type affects handling requirements: Open procedures allow broader material choice, while minimally invasive procedures require devices that are easier to deploy and control.
- Limited access affects knotting and manipulation: In laparoscopic or minimally invasive settings, ease of handling and secure fixation become critical considerations.
- Wound classification impacts material choice: Contaminated or infected wounds may influence selection due to differences in tissue response and material behavior.
4. Operational, Training, and Standardization Factors
Beyond clinical selection, healthcare systems must evaluate how closure devices fit within operational, financial, and standardization frameworks.
- Staff training and familiarity: Devices that align with existing surgical techniques reduce variability and training burden.
- Inventory and standardization requirements: Maintaining consistent stock across sizes and materials supports efficiency and reduces supply complexity.
- Workflow integration: Devices must align with surgical workflows, including ease of use, time efficiency, and post-operative management requirements.
Final Thoughts
Surgical closure is no longer just a technical step at the end of a procedure. It influences how consistently outcomes are achieved across different surgeons, settings, and patient profiles.
As absorbable wound closure device design changes, the focus is shifting toward reducing technique-dependent variability, improving repeatability, and aligning with real-world surgical workflows.
In this setting, systems such as SubQ It! SU-25 is subcuticular wound closure device designed to mechanically deploy absorbable fasteners beneath the skin.
These systems support consistent dermal approximation without removal, making them particularly relevant for procedures where both operative efficiency and standardization are priorities.
Get in touch with the team to explore how SubQ It! SU-25 fits into your surgical workflow, and learn more about this advanced system.
FAQs
1. How long do absorbable wound closure devices take to dissolve?
Absorption depends on the material used. Fast-absorbing sutures may dissolve within 7–14 days and are fully absorbed by 21 days.
2. Are absorbable wound closure devices as strong as traditional sutures or metal staples?
Yes, absorbable devices offer sufficient strength during early healing, after which their support gradually decreases as tissue stability improves. Different materials offer varying strength retention profiles depending on the clinical requirement.
3. What are the main differences between absorbable barbed sutures and absorbable subcuticular staplers?
Barbed sutures are manually placed and anchored within tissue without knots. Subcuticular staplers use a device to place absorbable fasteners beneath the skin in a consistent pattern. Sutures offer greater flexibility for complex wounds, while staplers provide standardized application in selected cases.
4. Can absorbable wound closure devices be used for all types of surgical incisions?
Absorbable devices are widely used for soft-tissue closure, but they are not suitable for every situation. High-tension or deep structural layers require materials with prolonged strength retention. Selection should be based on wound characteristics and healing requirements.
5. Do absorbable wound closure devices cost more than traditional closure methods?
Absorbable devices may have higher upfront costs compared to basic sutures or staples. However, they can reduce follow-up visits and eliminate removal procedures, which may offset overall resource use depending on the clinical setting.
6. What are the cosmetic outcomes with absorbable wound closure devices compared to metal staples?
Absorbable and non-absorbable methods achieve similar long-term cosmetic outcomes when proper technique is used. Subcuticular absorbable approaches may reduce surface marks by placing material beneath the skin, but results depend more on technique than material alone.
7. Are absorbable wound closure devices safe for use in contaminated or infected wounds?
Absorbable devices can be used in selected contaminated wounds, but the choice of material matters. Monofilament absorbable sutures are often preferred because they are less susceptible to bacterial adherence than braided materials.
8. Do absorbable wound closure devices affect surgical closure time?
Closure time varies by device type and surgeon familiarity. Systems such as barbed sutures or subcuticular staplers may reduce closure time by eliminating knot tying, whereas traditional sutures typically require more time.