The way an incision is closed directly affects operative flow, consistency of approximation, and overall wound healing.
As closure technologies continue to change, the global wound closure market is projected to reach USD 30.35 billion by 2035, reflecting sustained focus on improving outcomes and procedural efficiency.
With this increased emphasis, closure method selection is no longer a routine choice but a considered clinical decision. Sutures, staples, adhesives, and subcutaneous systems each carry different implications for speed, control, and cosmetic results.
In this blog, you’ll explore how surgeons choose types of skin closure in 2026 based on wound classification, tissue condition, incision features, and postoperative needs.
Key Takeaways:
- Skin closure technique selection affects operative efficiency, closure consistency, healing outcomes, and postoperative workflow, making it a key intraoperative decision.
- Methods such as sutures, staples, tissue adhesives, and subcutaneous systems differ in speed, control, tension management, and cosmetic outcomes.
- The closure approach depends on timing, with primary, secondary, and delayed closures selected based on contamination level and tissue condition.
- Key decision factors include wound classification, tissue viability, incision tension, anatomical location, and postoperative follow-up needs.
- Selection errors, such as ignoring contamination, underestimating tension, or prioritizing speed, can increase complication risk and affect outcomes.
What Are Skin Closure Techniques in Surgery?
Skin closure techniques are the methods surgeons use to approximate wound edges after an incision, influencing closure time, cosmetic outcomes, and overall OR (Operating Room) workflow.
In practice, closure method selection is part of intraoperative planning rather than a final step at the end of the procedure.
Surgeons evaluate closure techniques based on how they perform across key intraoperative factors:
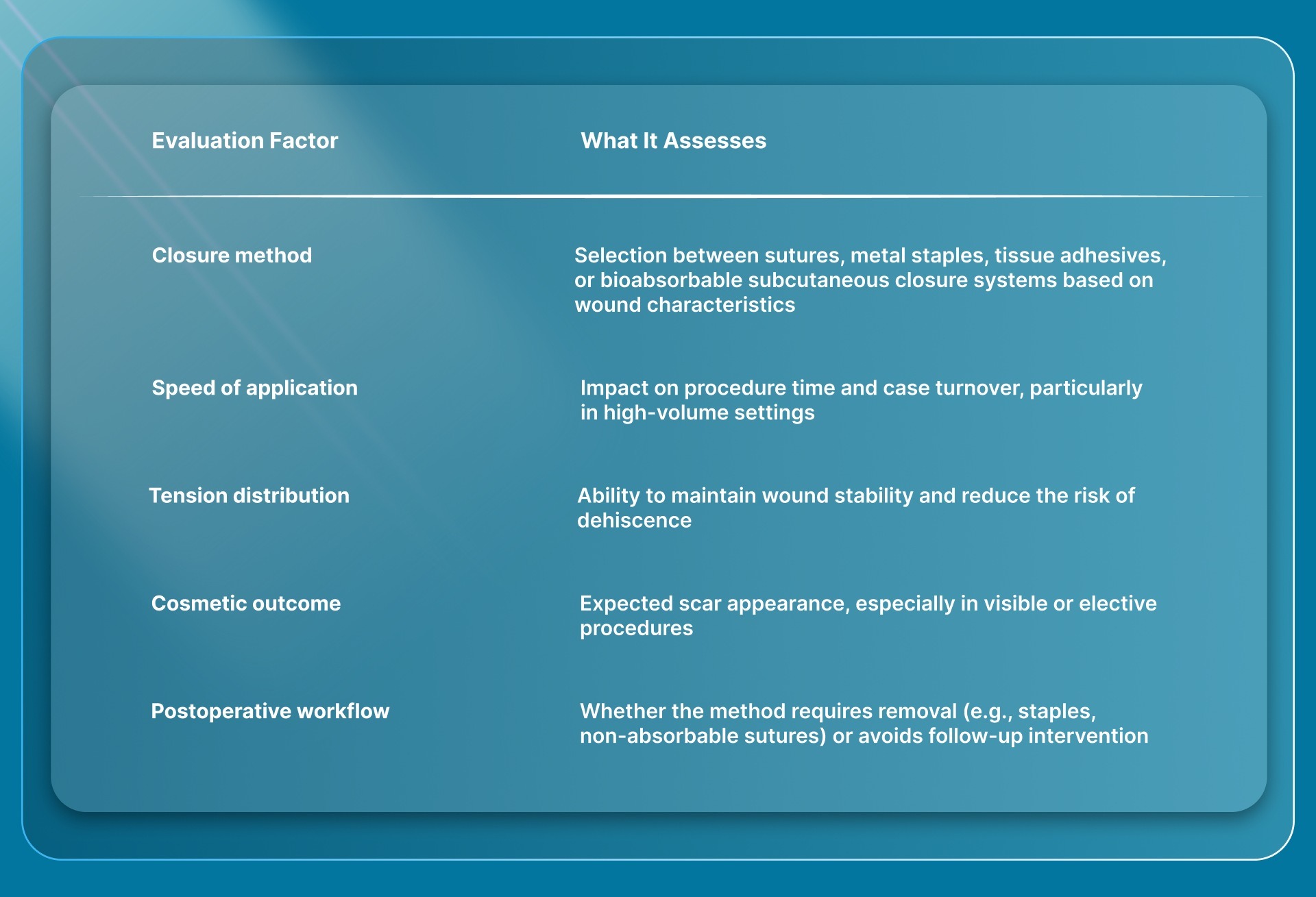
The choice of closure technique depends on incision type, anatomical location, and surgical context, with each method offering trade-offs in speed, control, and postoperative outcomes.
A clear understanding of available skin closure techniques helps explain why selecting the right method in the operating room directly influences surgical and postoperative outcomes.
Why Skin Closure Technique Selection Matters in the OR?
Skin closure directly affects operative flow, resource utilization, and downstream patient management. For surgeons, especially in private practice or high-volume settings, the choice of technique has a measurable impact beyond the incision itself.
Selecting the right technique influences key intraoperative and postoperative outcomes:

In practical terms, the closure method you choose can influence whether a case runs on schedule, whether additional follow-up is required, and how efficiently your practice operates over time.
Understanding why technique selection matters provides useful context for reviewing the different skin closure methods used in surgical practice.
4 Types of Skin Closure Techniques Used in Surgery
Surgeons have multiple skin closure options, each designed to address different intraoperative priorities such as speed, control, and cosmetic outcome.
Each technique performs differently depending on incision length, tissue tension, and procedural context.
The main types of skin closure techniques used in surgery include:
1. Sutures
Sutures allow precise approximation of skin edges with controlled tension and placement, making them a reliable option across a wide range of procedures.
They are commonly used when alignment and cosmetic outcome are important, particularly in areas where accuracy matters.
- High precision and control: Sutures allow surgeons to adjust each stitch individually, enabling accurate edge alignment and controlled eversion.
- Versatility across wound types: They are suitable for a wide range of tension conditions and are often combined with deeper-layered closure when required.
- Technique-dependent application: Placement requires skill and time, and outcomes can vary depending on the surgeon's technique.
- Removal considerations: Non-absorbable sutures require a follow-up visit for removal, which adds to the postoperative workflow.
2. Staples
Staples are mechanical devices used to rapidly approximate skin edges, particularly in longer incisions or time-sensitive procedures. They are often selected when speed and consistency are prioritized over fine cosmetic detail.
- Fast application in the OR: Staples can be placed quickly, reducing closure time compared to manual suturing.
- Consistent spacing and deployment: The device delivers uniform placement, minimizing variability across the incision.
- Postoperative removal required: Staples typically need to be removed within 7–14 days after healing, requiring an additional patient visit.
- Surface penetration and scarring: Because staples penetrate the skin surface, they can result in more visible scarring.
3. Tissue Adhesives
Tissue adhesives are topical agents that bond the skin surface without penetrating tissue, offering a non-invasive closure method. They are best suited for small, low-tension incisions where speed and patient convenience are priorities.
- Non-invasive application: Adhesives are applied externally, eliminating the need for needles or mechanical devices.
- No removal required: The material naturally sloughs off as the wound heals, avoiding the need for follow-up visits for removal.
- Limited tensile strength: Adhesives are not suitable for wounds under significant tension or stress.
- Restricted use cases: They are typically used for small, simple incisions rather than complex or high-tension closures.
4. Bioabsorbable Subcutaneous Closure Systems
Bioabsorbable subcutaneous systems place fasteners beneath the skin surface, offering an alternative to traditional surface-based closure methods. These systems aim to combine efficient deployment with subcuticular closure principles.
- Subcutaneous placement approach: Fasteners are designed to approximate tissue beneath the skin, avoiding epidermal penetration in systems built for subcuticular placement.
- No removal required: Bioabsorbable materials are gradually broken down by the body, eliminating the need for removal.
- Repeatable deployment: These systems allow consistent placement along the incision using a mechanical delivery mechanism.
- Applicability based on device design: Use depends on incision size and clinical context, with different variants designed for different lengths, including systems such as SubQ It! SU-25, which is used in longer incision closures.
In addition to the specific techniques used, wound closure can also be classified by the underlying healing approach that guides surgical decision-making.
3 Types of Wound Closure Based on Healing Approach
Not every incision is closed immediately. In many cases, the decision is about when to close the wound, based on contamination level, tissue viability, and intraoperative findings rather than the closure method itself.
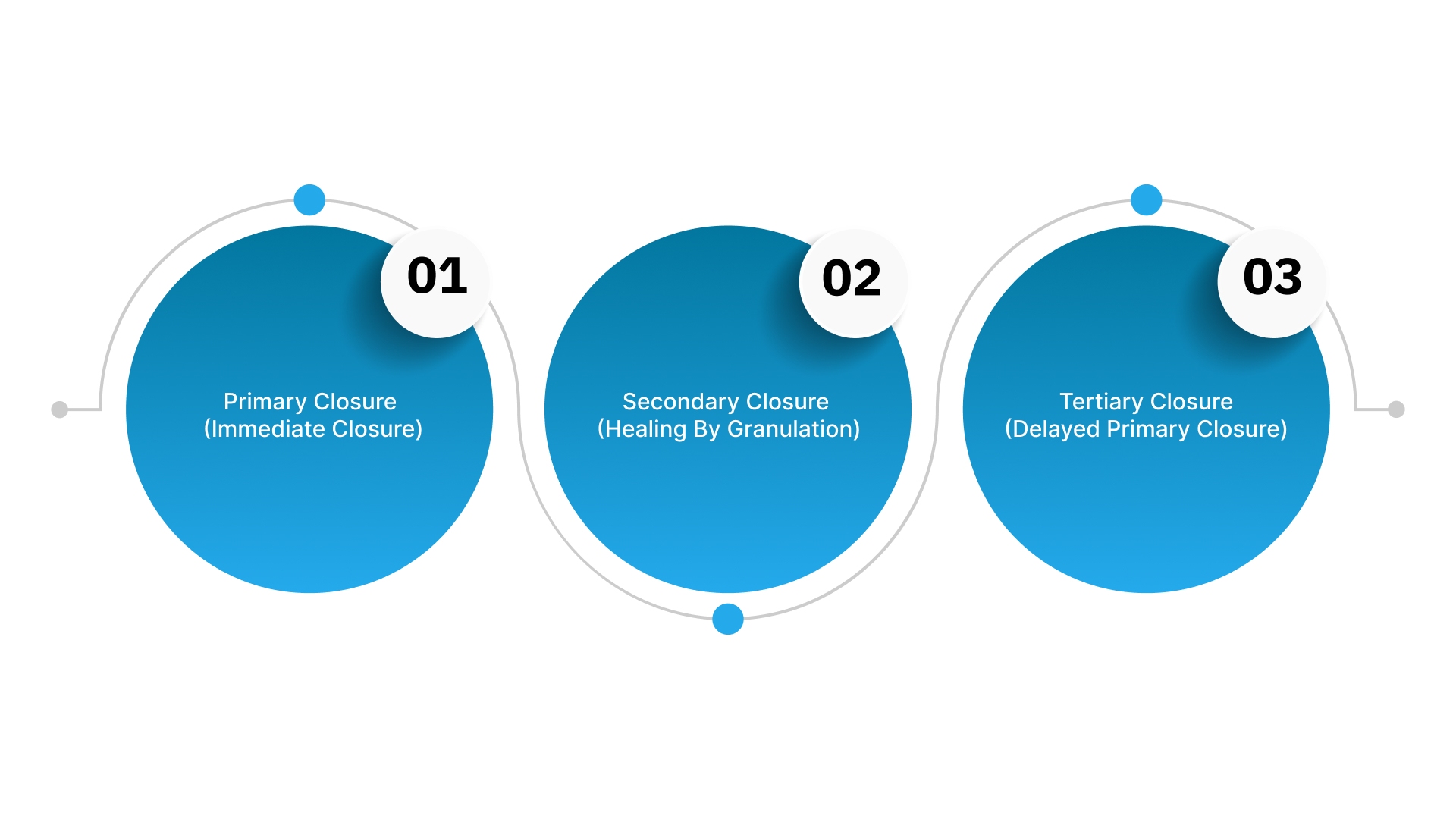
The three healing-based approaches define how closure is timed and managed:
1. Primary Closure (Immediate Closure)
Primary closure involves approximating wound edges at the time of surgery and is the standard approach for clean, controlled incisions. It is used when tissue is viable, and the risk of infection is low.
- Immediate wound closure: The incision is closed during the same procedure, allowing faster progression to epithelialization.
- Used in clean surgical settings: Most elective procedures and controlled operative environments follow this approach.
- Predictable healing profile: Healing is typically faster and more predictable compared to delayed or open approaches.
- Supports operative workflow completion: Enables closure within the same procedure without requiring staged management.
2. Secondary Closure (Healing by Granulation)
Secondary closure allows the wound to heal without surgical approximation, progressing through granulation tissue formation and epithelialization.
It is used when immediate closure would increase the risk of infection or when tissue loss prevents approximation.
- Wound left open intentionally: No immediate closure is performed, allowing natural healing from the base upward.
- Used in contaminated or tissue-loss scenarios: Appropriate when infection risk or inability to approximate edges prevents safe closure.
- Extended healing duration: Healing may take weeks to months, depending on wound size and depth.
- Larger and more contracted scars: Healing without edge approximation often results in broader or more contracted scars.
3. Tertiary Closure (Delayed Primary Closure)
Tertiary closure involves initially leaving the wound open, followed by closure after a short observation period. It is a staged approach used when immediate closure is uncertain due to contamination or edema.
- Delayed decision to close: The wound is reassessed after several days, then definitive closure is performed.
- Allows control of contamination and edema: Provides time to reduce infection risk and stabilize the wound environment before closure.
- A combination of open and surgical management: Integrates initial open management with later surgical approximation of wound edges.
- Used in higher-risk scenarios: Common in traumatic wounds, contaminated surgical fields, or cases with significant swelling.
The healing pathway influences closure strategy, which is why technique selection must align with the wound’s biological and clinical context.
How Surgeons Choose the Right Skin Closure Technique?
Selecting a skin closure technique is a case-specific decision, not a routine step. The choice depends on how well a method aligns with the incision characteristics, tissue condition, operative context, and expected postoperative course.
The decision is guided by a set of practical intraoperative factors:
1. Wound Classification and Contamination Level
The level of contamination determines whether immediate closure is appropriate. Clean and clean-contaminated wounds are typically closed during the same procedure, while contaminated or high-risk wounds may require delayed closure to reduce the risk of infection.
2. Tissue Condition and Viability
Successful closure depends on the quality of the tissue being approximated. Well-vascularized tissue supports reliable healing, while compromised tissue, such as ischemic or friable tissue, may increase the risk of breakdown and may not tolerate certain closure techniques.
3. Tension Across the Incision
Excessive tension can compromise wound stability and healing. If edges cannot be approximated without tension, alternative approaches such as layered closure or tension-distributing techniques are required to reduce the risk of dehiscence.
4. Anatomical Location and Visibility
Closure technique varies depending on anatomical location. High-visibility areas often require more precise approximation to support improved cosmetic outcomes, while lower-visibility areas may allow for faster methods depending on clinical priorities.
5. Incision Length and Procedural Context
The length of the incision and the nature of the procedure influence the selection of technique.
Longer incisions or time-sensitive cases may favor faster closure methods, while smaller or controlled incisions allow for more precise, technique-dependent approaches.
6. Postoperative Management Requirements
Different closure methods have different follow-up implications. Techniques that require removal introduce additional visits and workflow considerations, while others eliminate the need for postoperative removal, affecting both patient management and practice efficiency.
Even with a structured approach to technique selection, certain decision-making gaps can still lead to avoidable errors in skin closure practice.
Common Mistakes in Skin Closure Selection
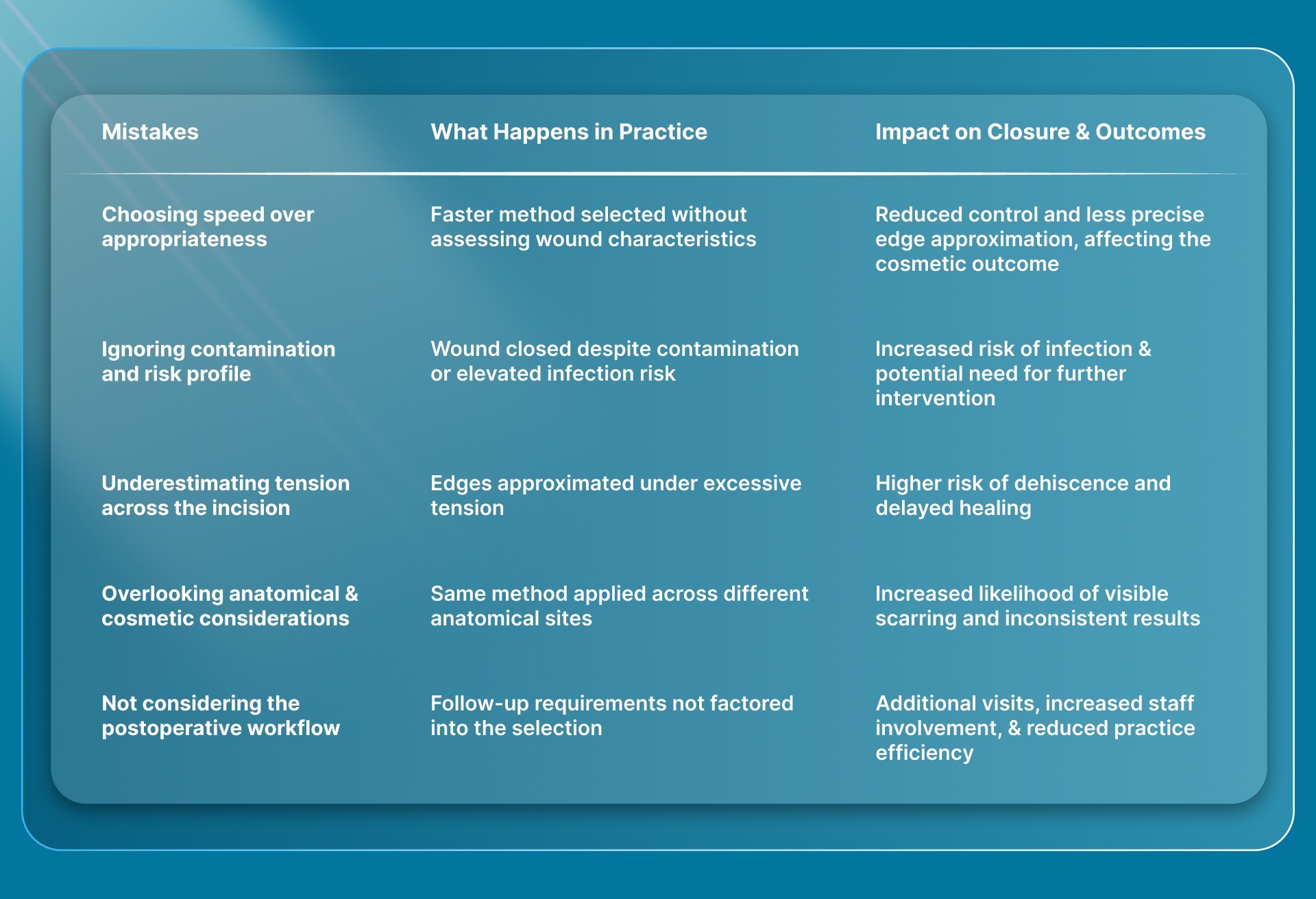
Skin closure decisions are often made under time pressure, but small misjudgments at this stage can affect healing, workflow, and patient outcomes.
These are not technique errors but selection errors in which the chosen method does not match the clinical scenario.
Final Thoughts
Skin closure decisions extend beyond approximation, influencing both outcome consistency and the efficiency with which cases are managed and reproduced across different operative settings.
As expectations for efficiency and consistency increase, closure methods that balance speed with controlled tissue approximation become more relevant in routine workflows.
In this context, SubQ It! SU-25 delivers 25 staples to close incisions up to 25 cm, covering cases that would otherwise require extended manual suturing.
It also saves approximately 25 minutes of OR time per procedure, supporting more efficient case flow.
Contact us to explore how SubQ It! SU-25 fits into your workflow and evaluates its role in improving closure efficiency and consistency.
FAQs
1. What are the types of wounds?
Wounds are classified as acute or chronic based on healing progression and by cause, such as surgical incisions, traumatic wounds, burns, or ulcers. In surgical practice, they are also categorized by contamination level as clean, clean-contaminated, contaminated, or dirty/infected.
2. How does incision location affect skin closure technique selection?
Incision location influences both tension distribution and expectations of cosmetic outcome, which directly affect technique choice. High-mobility or high-visibility areas typically require more precise, tension-controlled methods compared to less visible regions.
3. What are the key principles of wound closure?
Effective wound closure requires accurate tissue approximation, minimal tension, and preservation of blood supply to support healing. It also involves appropriate timing of closure, infection control, and technique selection based on wound characteristics.
4. When should absorbable vs non-absorbable closure methods be used?
Absorbable methods are used when removal is not practical or when minimizing follow-up is important, while non-absorbable options are selected when prolonged external support is required. The choice depends on wound type, location, and postoperative management needs.
5. What are the wound closure techniques?
Wound closure techniques include sutures, staples, tissue adhesives, and bioabsorbable subcutaneous closure systems used to approximate skin edges. These methods differ in speed, precision, tension control, and postoperative requirements, depending on the clinical scenario.
6. What role does the closure technique play in scar formation?
Closure technique affects how evenly wound edges are approximated and how tension is distributed across the incision. Poor alignment or excessive tension can lead to wider or more visible scars, whereas appropriate technique selection can improve cosmetic outcomes.