Suture clips have been a staple of wound closure for decades. They're fast to apply, consistent in tension, and familiar to every trained surgeon. Yet the tradeoffs have stayed the same. Removal visits, surface puncture marks, and cosmetic limitations that patients increasingly notice.
In a study of liver resection patients, raised scars appeared in 9.4% of subcuticular closures compared to 25.9% of surface-stapled closures. The cosmetic advantage of keeping closure materials under the skin is measurable and well-documented.
This post breaks down the different suture clip types available today, their limitations, and the newer bioabsorbable options that are changing how closures get done.
Key Takeaways
- Suture clips include metal skin clips, absorbable laparoscopic clips, ligating clips, and bioabsorbable subcutaneous fasteners, each designed for a different clinical purpose.
- Traditional metal clips require a removal visit at 7 to 10 days and leave characteristic railroad-track scars from surface puncture points.
- Surface staples carried a 5.9% deep infection rate versus 1.4% for subcuticular closure.
- Bioabsorbable subcutaneous fasteners are made from a polylactide-polyglycolide copolymer that dissolves over 90 to 120 days, requiring no removal visit.
- OR operating costs range from $22 to $133 per minute, depending on the facility, making closure time a direct economic variable for high-volume practices.
What Are Suture Clips?
Suture clips are mechanical devices that hold wound edges together as an alternative to hand-tied stitches. They work by applying consistent, evenly distributed tension across the incision line, which reduces variability in closure quality.
The category has expanded well beyond its original form. Surgeons today can choose from stainless steel skin clips for external approximation, absorbable polymer clips for internal tissue handling, and bioabsorbable fasteners that go entirely under the skin. Each type targets a different layer of tissue and a different clinical need.
What separates clips from thread-based sutures is the mechanism. Sutures require knot-tying, which introduces variability based on technique and tension. Clips apply a fixed, reproducible force, which is one reason they've remained popular for high-volume closures.
What Types of Suture Clips Do Surgeons Use Today?
Suture clips range from stainless steel skin closure devices to polymer-based fasteners that dissolve under the skin. Each type targets a different tissue layer and a different clinical goal.
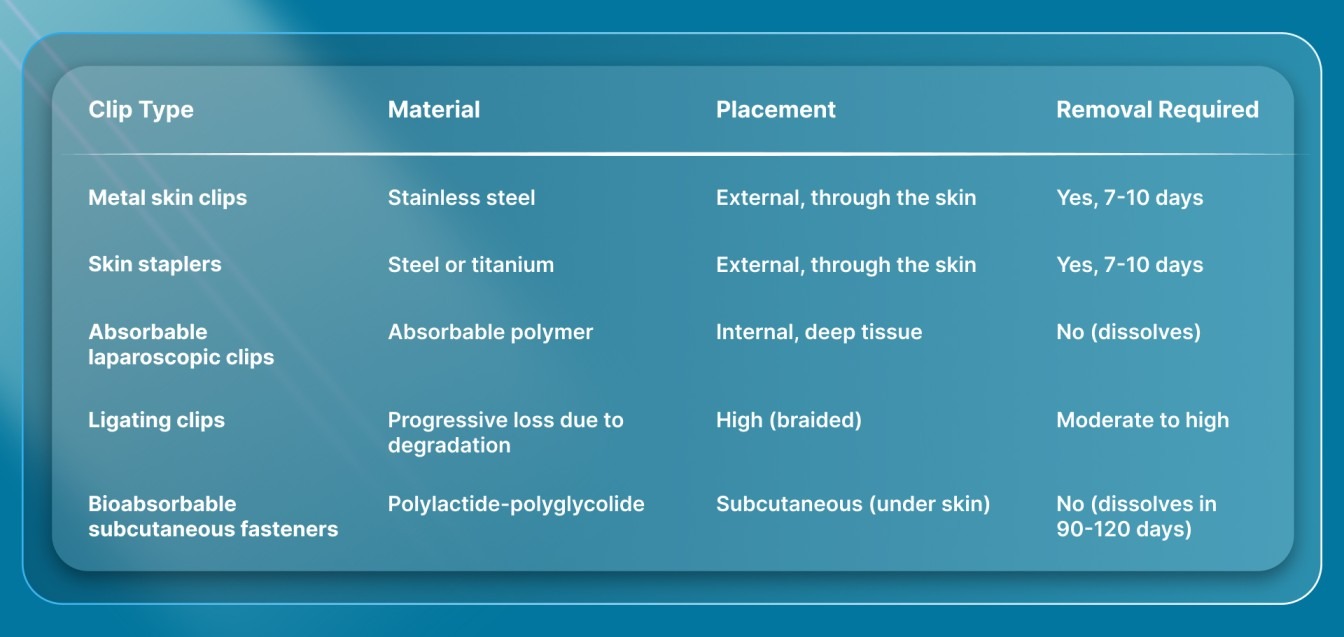
Here's how the main categories compare at a glance. Each category works differently in practice. Here’s a closer look at what separates them:
Metal Skin Closure Clips
Michel clips are the oldest and most recognized type. Made from stainless steel, they approximate skin edges from the
Clips aren't universally superior. Complex flaps, high-tension closures, and outside by clamping across the wound. They're applied and removed with dedicated forceps.
Standard skin staplers fall into this same category. They fire stainless steel or titanium staples through the skin surface, holding the wound closed mechanically. Both Michel clips and skin staplers share the same core limitation: they pierce the skin surface, require removal in 7 to 10 days, and leave railroad-track scars at each puncture site.
Absorbable Laparoscopic Clips
Lapra-Ty clips and similar devices are used inside the body during laparoscopic procedures. They secure absorbable suture ends without hand-tied knots, which saves time during deep tissue surgery where knot-tying is slow or impractical.
Ligating Clips
Ligating clips control blood vessels, not skin. Made from titanium or polymer, they're applied to vessel stumps or duct ends during dissection. These are also a type of suture clip, but they serve a completely different purpose than wound closure.
Bioabsorbable Subcutaneous Fasteners
This is the newest category. Bioabsorbable subcutaneous fasteners are placed entirely beneath the skin surface, in the dermal layer. They're made from a polylactide-polyglycolide copolymer that dissolves over 90 to 120 days once fired.
The fasteners go under the skin rather than through it, so they leave no surface puncture marks and require no removal visit. This category covers incisions from a few millimeters (small laparoscopic trocar sites) up to 25 cm (open surgical procedures), depending on the device variant.
Why Do Surgeons Choose Clips Over Hand-Sewn Sutures?
Clips offer a combination of speed and consistency that hand-tied sutures can't always match. The practical reasons come down to how closure time, technique variability, and safety risks play out across a full surgical schedule.
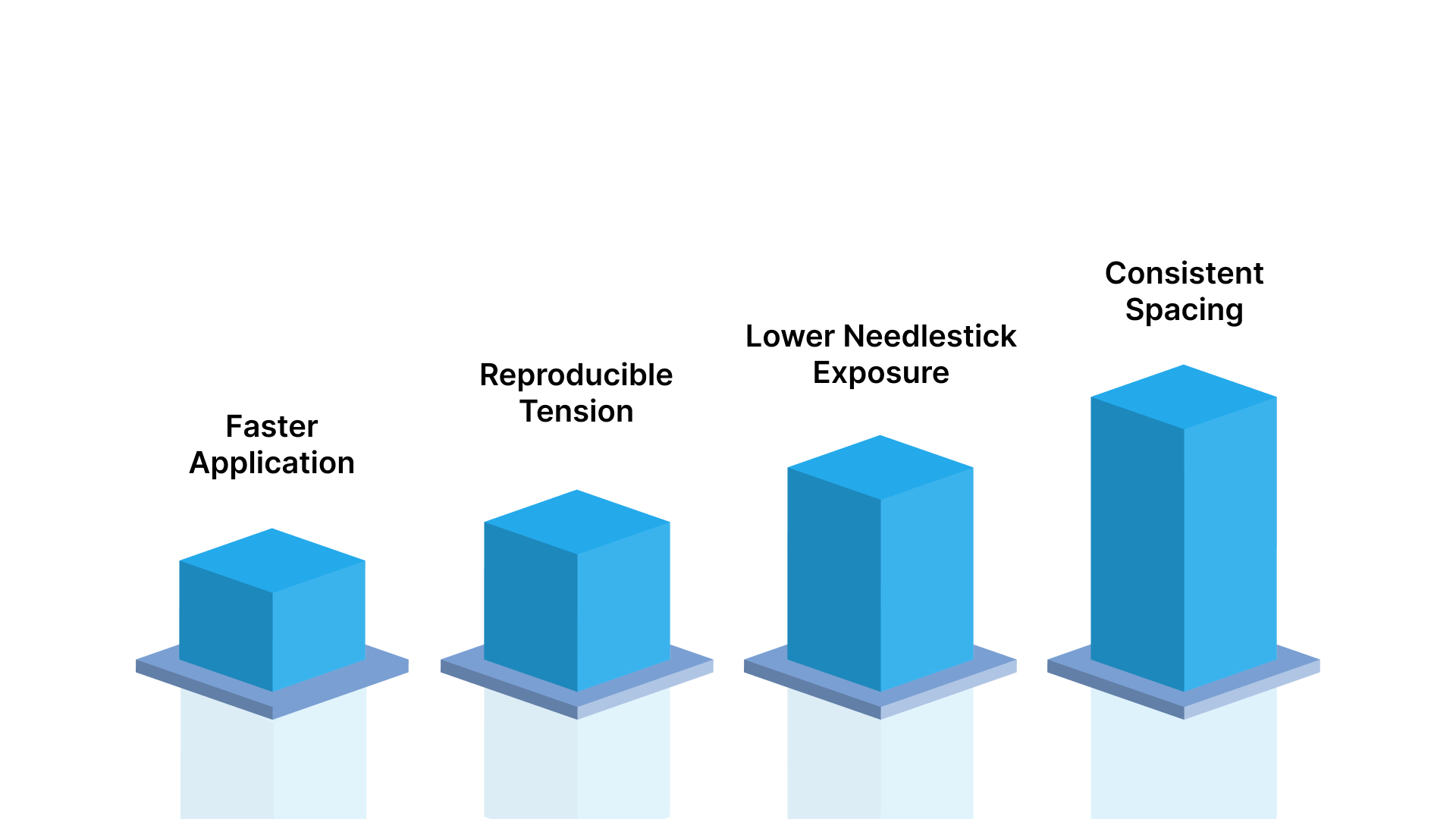
- Faster application: Metal clips and staplers close wounds in a fraction of the time required for running subcuticular stitches. In bilateral breast reductions, an absorbable stapler cut closure time by 21.8 minutes on average compared to hand-sewn sutures. After adjusting for tissue volume and pedicle technique, the difference widened to 26.5 minutes.
- Reproducible tension: Every clip applies the same mechanical force. Hand-tied knots vary with surgeon fatigue, technique, and speed, introducing inconsistency across long closures.
- Lower needlestick exposure: Suturing requires repeated needle passes through tissue. In one observational study of 106 surgical physicians, 18.87% sustained at least one needlestick injury during a six-month window. The highest share of those injuries, 65%, occurred during closure of incisions longer than 10 cm. Clip-based systems reduce needle handling during the closure phase.
- Consistent spacing: Clip devices fire at regular intervals, producing evenly spaced closure points. Hand-sewn sutures depend on the surgeon maintaining uniform bite depth and spacing along the entire incision.irregular wound geometries still favor hand-sewn techniques where the surgeon can adjust tension dynamically. The advantage of clips is most pronounced in straightforward, linear skin closures where speed and consistency matter.
What Are the Limitations of Traditional Metal Suture Clips?
Metal clips close wounds quickly, but the tradeoffs have remained essentially unchanged since the devices were introduced. Three limitations consistently arise in clinical practice.
- Mandatory removal visit: Metal clips and surface staples must come out within 7 to 10 days. For the patient, that's an extra appointment. For the practice, it's scheduling time, staff allocation, and a procedure room occupied for a non-revenue task. Every staple removal visit carries this overhead.
- Railroad-track scarring: Surface clips pierce the skin at each application point, leaving paired puncture marks on both sides of the incision line. These transverse scars are visible, permanent, and a frequent source of patient dissatisfaction, especially in cosmetically sensitive areas.
- Higher infection signals in some data: A Harvard/Massachusetts General Hospital review of open posterior lumbar cases found deep surgical site infections in 5.9% of incisions closed with surface staples versus 1.4% in those closed with a running subcuticular absorbable stitch. The subcuticular group actually carried higher baseline risk, with more revision cases and instrumented fusions, making the difference more notable.
These limitations don't make metal clips unusable. They remain a practical choice for scalp lacerations, orthopedic closures where cosmesis is secondary, and situations where speed overrides all other considerations. The question is whether the tradeoffs are acceptable for the specific case, patient population, and practice setting.
How Do Bioabsorbable Clips Compare to Metal Clips for Skin Closure?
SubQ It! is a bioabsorbable wound closure system that places dissolving dermal fasteners subcutaneously (under the skin) to close incisions. Unlike traditional metal clips that pierce the skin surface, these fasteners go into the dermal layer and break down naturally over 90 to 120 days without requiring removal or leaving surface puncture marks.

Here's how the two approaches compare across key clinical outcomes. Each of these differences is backed by published clinical data. The sections below walk through the evidence.
Scarring Outcomes
In a study of 85 pairs of liver resection patients, raised and thickened scars appeared in 9.4% of subcuticular closures versus 25.9% of those closed with surface staples. The subcuticular group also had a shorter median hospital stay of 10 days compared to 15 days.
This aligns with the mechanism's predictions. When closure materials stay beneath the skin surface, there's no external puncture trauma to generate the railroad-track scarring pattern that surface clips produce.
Closure Time
Speed has historically been the argument for metal clips over hand-sewn closure. Bioabsorbable skin closure systems are changing that equation. In Columbia University's review of 62 patients, an absorbable stapler finished closure faster than hand-sewn sutures on average, and wound healing complication rates were similar between the two approaches.
For practices running multiple cases per day, that time savings is meaningful. It's also time recovered without a corresponding loss in wound integrity.
Infection Rates
The spine data on surface staples and deep infection rates reinforces the broader trend favoring subcuticular approaches. A separate analysis of 31,419 cesarean deliveries at Tel Aviv Sourasky Medical Center found that absorbable subcutaneous staples produced the shortest total procedure time at 52 minutes, compared to 53 minutes for non-absorbable staples and 60 minutes for subcutaneous sutures. Infection rates during the 45-day follow-up did not differ across the three groups.
After adjusting for confounders, the absorbable subcutaneous staple group in that cesarean cohort also had lower odds of prolonged hospitalization beyond 5 days and lower odds of readmission within 45 days compared to the non-absorbable staple group.
When Should Surgeons Consider Bioabsorbable Fasteners Over Metal Clips?
The decision depends on the case mix, the patient population, and the practice model. Three clinical scenarios consistently favor the bioabsorbable subcutaneous approach.
Cosmetically Sensitive Procedures
Plastic surgery, facial closures, and any case where the patient's scar visibility matters to outcomes or satisfaction. Surface clips leave railroad-track marks that are difficult to revise. Subcutaneous tissue fasteners avoid external puncture entirely, leaving only the original incision line.
The liver surgery data confirms the cosmetic advantage isn't limited to plastic surgery. It holds across surgical specialties where closure technique is the variable.
Laparoscopic and Minimally Invasive Cases
Small trocar-site incisions (a few millimeters) are difficult to close with surface clips or standard skin staplers. The incision is often too small for the device to operate effectively. SubQ It! SU-10 places 10 bioabsorbable fasteners and closes incisions up to 10 cm, including very small laparoscopic port sites where surface-applied devices can't function. Zipper-style external devices also can't serve these small incisions.
High-Volume Private Practices
When OR time directly affects case throughput, the closure time reductions documented in plastic surgery data matter financially. OR costs per minute vary widely by facility, and for a private clinic running five or six cases a day, saving 20 minutes per closure can open room for additional procedures.
The removed follow-up visit is a separate efficiency consideration. Every follow-up appointment that doesn't need to happen frees scheduling capacity, staff time, and room availability.
What Do Suture Clips Cost Surgeons in OR Time?
Closure time is a cost line item. The time a surgeon spends closing an incision is time the OR is occupied, the anesthesia team is engaged, and the next case is waiting.
Duke University researchers documented OR expenses ranging from $22 to $133 per minute, depending on facility type, and noted that operating rooms account for roughly 40% of a hospital's total revenue. At even the lower end of that range, a 20-minute reduction in closure time represents a meaningful cost difference per case.
Metal clips are faster than hand-sewn subcuticular closure, but they incur downstream costs that don't appear on the OR ledger. The removal visit, staff time, patient scheduling, and occasional complications from delayed removal all add up across a full surgical calendar.
Bioabsorbable subcutaneous fasteners remove the downstream removal cost entirely. The large cesarean cohort data showed that absorbable subcutaneous staples produced the fastest total procedure times and lower rates of prolonged hospitalization, suggesting the time advantage extends beyond the OR itself.
For private-practice surgeons who own their scheduling and directly feel the financial impact of OR throughput, selection of closure method is an economic decision as much as a clinical one.
Final Thoughts
Suture clips have evolved from a single stainless steel device into a category with distinct subcategories, each suited to different clinical needs. Metal skin clips and surface staplers remain practical for cases where speed is the priority and cosmetic outcome is secondary. Bioabsorbable subcutaneous fasteners represent the newest branch of the category, offering measurable advantages in scar formation, infection rates, and follow-up burden.
The right clip choice depends on your case mix, your patients' cosmetic expectations, and how your practice values OR time. Reviewing the clinical data across specialties gives a clearer picture of where each option performs best and where the tradeoffs no longer need to be accepted.
SubQ It! places bioabsorbable fasteners under the skin to close incisions from a few millimeters up to 25 cm. The fasteners dissolve with no removal visit, no surface scarring, and better closure speeds. Contact us today to discuss how it fits your practice.
FAQs
1. How Long Do Bioabsorbable Suture Clips Take to Dissolve?
Bioabsorbable subcutaneous fasteners typically break down over a 90 to 120-day window. The polylactide-polyglycolide copolymer gradually degrades as the wound heals, and no removal appointment is needed.
2. Can Suture Clips Be Used on Curved or Irregular Incisions?
Yes, some clip types accommodate curved wound edges better than others. Metal skin clips work best on linear incisions, while subcutaneous fasteners placed in the dermal layer can follow slight curves along the incision path.
3. How Are Metal Suture Clips Removed After Surgery?
Metal clips are removed with a specialized clip remover or forceps at the 7 to 10-day follow-up visit. The clinician positions the remover under each clip, squeezes to open the clip arms, and lifts it free from the skin.
4. Do Suture Clips Interfere With Postoperative Imaging?
Metal clips made from stainless steel or titanium can produce artifacts on MRI and CT scans. Bioabsorbable polymer-based fasteners produce no imaging interference because they contain no metallic components.
5. Can Clips and Sutures Be Combined in the Same Closure?
Yes, combining techniques is common in layered closures. A surgeon might close deeper tissue layers with absorbable sutures and then approximate the skin with clips or subcutaneous fasteners, depending on the incision and cosmetic requirements.
6. Are There Incision Size Limits for Suture Clips?
Each device has a specified range. Metal skin clips work across a broad range of incision lengths, while bioabsorbable subcutaneous systems come in variants designed for specific sizes, from small laparoscopic port sites to incisions up to 25 cm.