In minimally invasive surgery, access constraints directly influence the efficiency with which each step can be performed. Working through a 5mm port limits instrument positioning, directly affecting control during tissue transection.
Even small differences in access strategy carry clinical relevance, with trocar-site hernia rates reported at up to 1.1% depending on port management.
In pediatric and anatomically restricted adult cases, instrument size often determines whether stapling can proceed without altering the port plan. Traditional 10–12 mm staplers may require upsizing, adding steps, and reducing maneuverability in tight fields.
A 5mm laparoscopic stapler addresses this by enabling controlled transection through a smaller access profile while maintaining procedural continuity.
In this blog, you’ll examine how surgeons use a 5mm laparoscopic stapler in 2026, including its performance in confined anatomy, procedure selection, and the technical factors that determine safe deployment.
Key Takeaways:
- 5mm laparoscopic staplers allow internal tissue transection through standard 5mm ports, avoiding port upsizing and maintaining minimally invasive access.
- These staplers provide better control and visibility in confined spaces such as the pelvis, thoracic cavity, and pediatric abdomen.
- 5mm laparoscopic staplers require multiple firings for longer resections, making precise staple line alignment critical to avoid gaps or weak junctions.
- Safe use of these staplers depends on correct tissue thickness, adequate compression, and proper positioning before each firing.
- 5mm laparoscopic staplers are less effective for thick tissue or long continuous transections, where larger staplers may be more efficient.
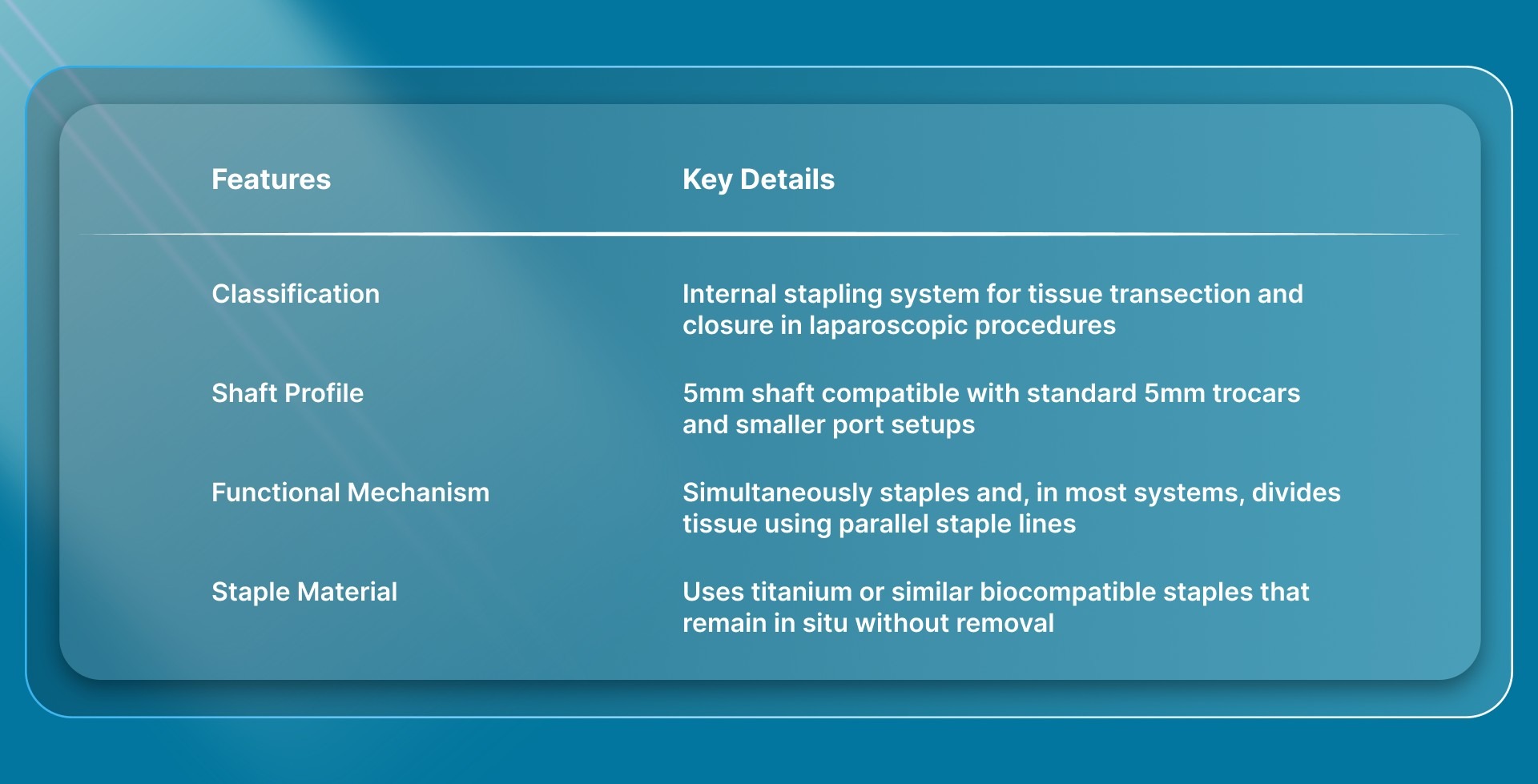
What Defines a 5mm Laparoscopic Stapler in Clinical Practice?
A 5mm laparoscopic stapler is defined by its ability to perform internal tissue stapling and, in most systems, simultaneous division through a 5mm access platform. In many cases, this can be done without changing the standard port setup.
In clinical practice, this definition is driven by access constraints, where instrument size determines whether stapling can be performed within an existing minimally invasive approach.
The structural and functional aspects outlined above directly influence its performance in limited working areas.
How Does a 5mm Laparoscopic Stapler Perform in Confined Anatomical Spaces?
In confined anatomy, performance is determined by how precisely you can position, align, and fire the device without compromising surrounding structures.
A 5mm laparoscopic stapler is chosen in these situations because it allows you to work within a limited space while maintaining control over staple placement and tissue handling.
Here’s how a 5mm laparoscopic stapler performs in confined anatomical spaces:
1. Access and Instrument Navigation
In tight spaces, the primary advantage is instrument entry and navigation without enlarging access points.
- Passes through existing 5mm ports, avoiding additional access trauma
- Reduces instrument crowding when multiple tools are in use
- Allows smoother navigation in narrow cavities such as the pelvis or pediatric abdomen
This is particularly relevant when larger instruments restrict movement or limit reach within the operative field.
2. Visual Field Preservation
In confined anatomy, maintaining a clear operative view is critical for safe stapling.
- A smaller shaft profile results in less obstruction of the camera view
- Improves visibility of target tissue and adjacent structures
- Allows more precise placement without repeatedly repositioning the scope
This influences how confidently you can align the device before firing.
3. Tissue Positioning and Alignment
Accurate alignment becomes more demanding as space decreases, and device size plays a direct role.
- Facilitates alignment in restricted angles without excessive manipulation
- Helps maintain tissue orientation without distortion during placement
In confined spaces, even small adjustments in positioning can determine staple line accuracy.
4. Control During Firing
Execution in tight anatomy depends on maintaining stability during the firing sequence.
- Reduced instrument bulk improves control when closing jaws and firing
- Minimizes unintended movement caused by limited working space
- Allows more controlled deployment when working near critical structures
These same access constraints also apply when managing small incisions at the end of the procedure.
Systems like SubQ It! SU-10, designed for incisions up to 10 cm, follows a similar principle by enabling subcuticular closure without the need for larger external devices.
These spatial considerations become even more apparent when evaluating how 5mm and 12mm staplers differ during active procedures.
5mm vs 12mm Laparoscopic Staplers: What Changes Intraoperatively?
The choice between a 5mm and 12mm laparoscopic stapler influences how you plan access, sequence the procedure, and execute stapling within the operative field.
The table below outlines the changes that occur during the procedure based on the stapler used.

These intraoperative differences also help identify the procedures where a 5mm stapler offers the greatest practical advantage.
5 Procedures That Benefit Most from a 5mm Laparoscopic Stapler
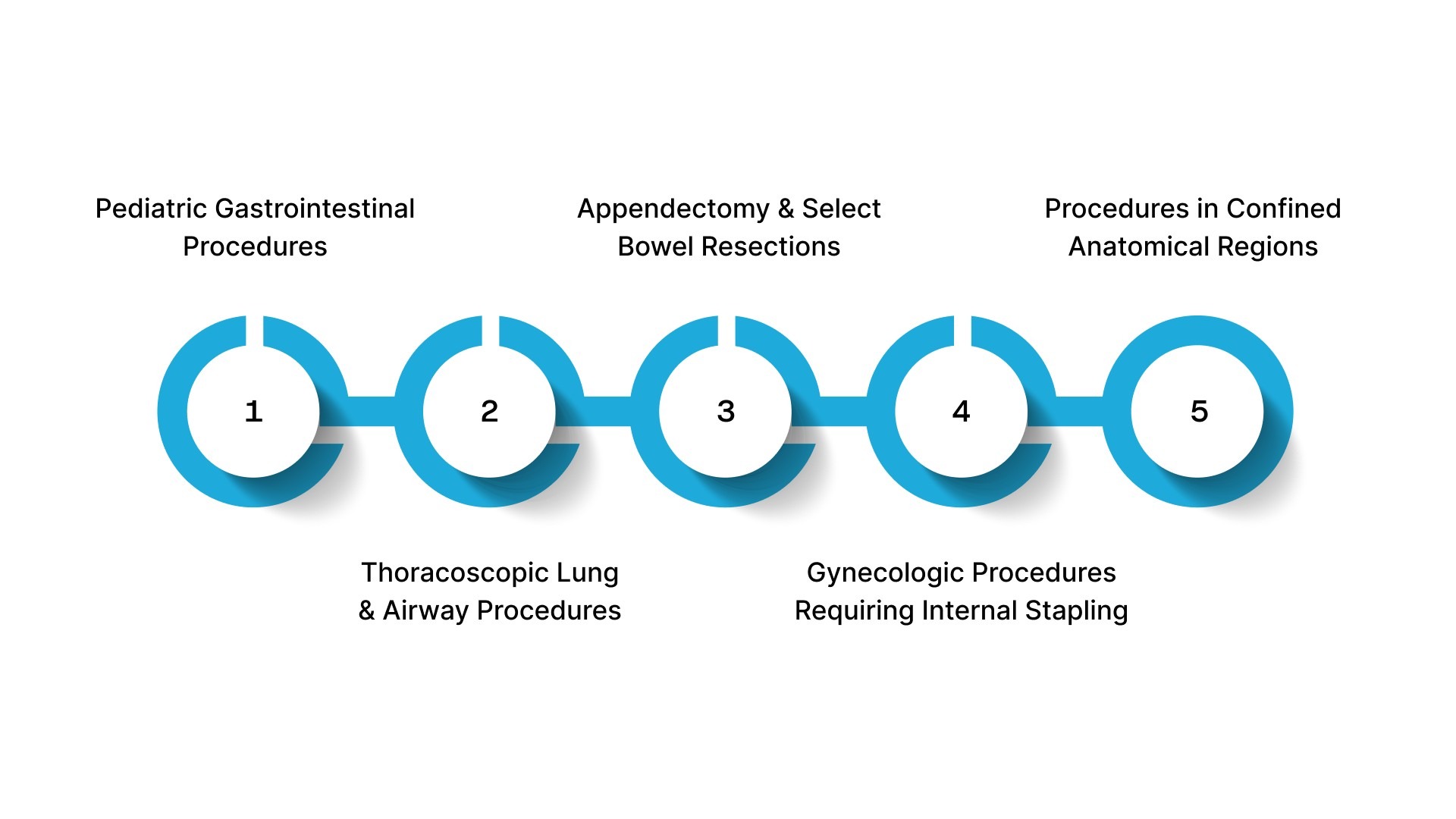 Procedure selection comes down to where a 5mm stapler fits naturally into your case without forcing changes to access or sequencing. Below are the procedures that benefit most from a 5mm laparoscopic stapler.
Procedure selection comes down to where a 5mm stapler fits naturally into your case without forcing changes to access or sequencing. Below are the procedures that benefit most from a 5mm laparoscopic stapler.
1. Pediatric Gastrointestinal Procedures
In pediatric cases, port size and working space are limited from the outset. A 5mm stapler allows you to stay within a small-port setup while completing key transection steps.
- Enterostomy takedown and small bowel resection
- Side-to-side bowel anastomosis in a limited abdominal space
- Procedures in neonates and infants where larger ports are not practical
2. Thoracoscopic Lung and Airway Procedures
A 5mm stapler can support the vessel and bronchial division without introducing larger instruments into a confined chest cavity.
- Thoracoscopic lobectomy
- Division of segmental vessels and bronchi
- Management of congenital lung lesions
3. Appendectomy and Select Bowel Resections
For simple GI cases, a 5mm stapler can be used in selected cases where tissue size and access allow controlled stapling within a smaller port strategy.
- Stapled appendiceal base division in selected cases
- Limited small bowel resections where access and tissue allow
- Selected colonic segments where tissue thickness is appropriate
4. Gynecologic Procedures Requiring Internal Stapling
In minimally invasive gynecologic surgery, maintaining smaller ports can be important for both access and cosmetic considerations.
- Ovarian cystectomy, where stapled transection is appropriate
- Selected hysterectomy steps where stapled transection is used
- Procedures where the instrument size directly affects access and visibility
5. Procedures in Confined Anatomical Regions
Certain cases are defined less by specialty and more by restricted working space, where instrument size becomes the deciding factor.
- Deep pelvic procedures with limited maneuvering room
- Small abdominal cavities in pediatric or low-BMI patients
- Situations where larger staplers restrict positioning or access
The value of a 5mm stapler in specific procedures depends equally on how well key technical parameters are managed.
5 Technical Factors That Determine Safe Use of a 5mm Laparoscopic Stapler
Safe use depends on whether the device is applied within its mechanical limits and the tissue behaves as expected at the moment of firing.
Below are the technical factors that determine safe use of a 5mm laparoscopic stapler.
1. Tissue Thickness Within Device Range
Tissue must fall within the specified compression range for reliable staple formation.
- Close the jaws gently and assess whether the tissue compresses evenly without resistance.
- Avoid tissue that is edematous, fibrotic, or thickened, as compression may be inadequate.
- Do not proceed if tissue appears over-compressed or excessively thin
2. Correct Tissue Placement Within the Jaws
Safe stapling requires that the tissue be fully and symmetrically positioned between the cartridge and anvil.
- Avoid partial capture of tissue at the edge of the jaws
- Ensure tissue is not twisted, folded, or under tension
- Maintain a clear view of the entire staple line before firing
3. Staple Line Alignment Across Sequential Firings
When multiple firings are required, alignment becomes a critical factor.
- Ensure each firing continues in line with the previous staple line
- Avoid overlapping or crossing staple lines, especially at junction points
- Pay close attention to the “crotch” area in anastomosis closures, where leaks can occur
4. Hemostasis and Immediate Reinforcement
Even with correct technique, minor bleeding can occur and must be addressed immediately.
- Use low-setting electrocautery for minor oozing
- Place reinforcement sutures if staple integrity is uncertain
- Control mesenteric or adjacent vessel bleeding as needed
5. Device Loading and Firing Readiness
Proper device setup is essential before introducing it into the operative field.
- Confirm the cartridge is correctly loaded and seated
- Ensure the mechanism cycles smoothly before use
- Avoid firing if there is any resistance or uncertainty in deployment
Even when these technical factors are carefully managed, certain practical limitations still remain in real surgical settings.
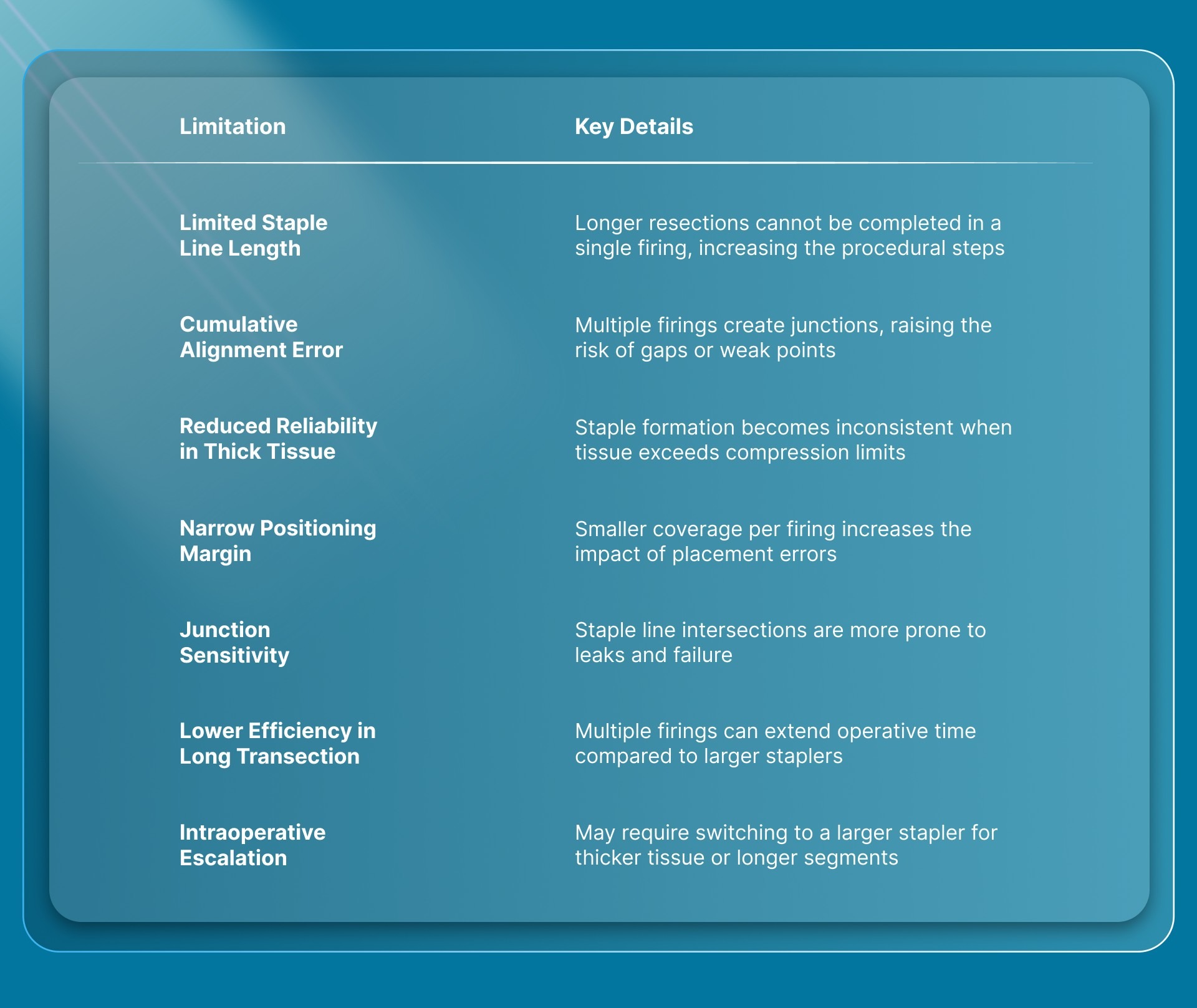
Limitations of a 5mm Laparoscopic Stapler in Real Surgical Settings
Limitations become apparent when the device is used outside its mechanical envelope or tissue compatibility range. Below are the key limitations of a 5mm laparoscopic stapler in real surgical settings.
Final Thoughts
In practice, the choice of stapler depends on access constraints, tissue characteristics, and the efficiency required to complete sequential transections.
Choosing the right stapling approach affects how efficiently you complete tissue transection in minimally invasive procedures. It also shapes how smoothly you transition into the final step of closure.
In laparoscopic cases using 5mm ports, closure systems such as SubQ It! SU-10 can be used for subcuticular approximation of incisions up to 10 cm without external staples.
Because the fasteners are bioabsorbable and placed subcutaneously, no removal visit is required.
Contact us to explore how SubQ It! SU-10 can support efficient closure and improve workflow in minimally invasive procedures.
FAQs
1. What are the main advantages of 5mm staplers over traditional 10mm staplers?
5mm staplers can reduce the need to upsize ports, potentially lowering access-related trauma and improving maneuverability in confined spaces. In selected procedures, they can also shorten stapled steps compared to hand-sewn techniques.
2. Can 5mm staplers be used in adult patients or only in pediatric cases?
Although developed for pediatric use, 5mm staplers can be used in selected adult cases, particularly in small bowel surgery or confined anatomy. Suitability depends on tissue characteristics and device-specific compression limits.
3. What complications should I watch for when using 5mm laparoscopic staplers?
Complications include anastomotic leaks at staple-line junctions, bleeding due to inadequate hemostasis, and incomplete staple formation caused by inappropriate tissue thickness.
4. How much training is required to become proficient with 5mm stapling techniques?
Device-specific training on loading and firing is essential, followed by simulation practice and initial supervised cases. Proper training reduces errors such as misloading and incorrect positioning.
5. Are 5mm staplers cost-effective compared to traditional methods?
In specific procedures such as enterostomy takedown, stapled techniques have shown reduced operative time and shorter hospital stays compared to hand-sewn methods. This can improve Operating Room (OR) efficiency, depending on the case.
6. What tissue thicknesses are appropriate for 5mm staplers?
Tissue must fall within the device’s compression range, depending on the stapler. Tissue outside this range requires alternative methods or larger staplers.