In laparoscopic surgery, instrument choice directly affects tissue control and preservation. When the grasper design does not align with tissue characteristics, the risk of unintended force or injury increases, particularly with limited tactile feedback.
Reported complication rates range from 1.49% to 31.58%, with vascular injuries accounting for 30% to 64% of severe complications. Although multifactorial, these outcomes are closely linked to tissue handling and instrument control.
Because procedures are performed through trocar access with indirect visualization, the design of the grasper remains central to precision and efficiency.
In this blog, you’ll explore the types of laparoscopic graspers and how to select the appropriate instrument for specific tissue and procedural requirements.
Key Takeaways:
- Laparoscopic graspers enable controlled tissue manipulation through 5–10 mm ports, where limited tactile feedback makes selection critical for precision and safety.
- Different grasper types serve specific roles, with dissecting, atraumatic, traumatic, and organ-specific designs matched to tissue and task.
- Tissue delicacy, thickness, and moisture influence instrument choice, affecting grip stability, force application, and injury risk
- Ergonomics, including handle design, locking mechanisms, and access angles, affect control and surgeon fatigue during procedures.
- Consistent instrument selection across surgical phases helps reduce variability and supports predictable operative outcomes.
What Is a Laparoscopic Grasper?
A laparoscopic grasper is a long, slender surgical instrument with hinged jaws at the distal tip, used to grasp, hold, and manipulate tissue during minimally invasive procedures.
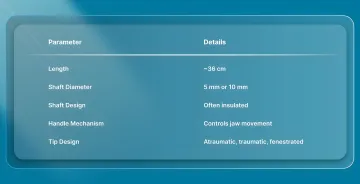
Key specifications and components include:
- Length: Typically 36 cm in standard adult laparoscopic procedures, allowing access through trocar ports
- Shaft diameter: Most commonly 5 mm or 10 mm, depending on port size and procedural requirements
- Shaft design: Often insulated when used with electrosurgical energy systems
- Handle mechanism: Transmits surgeon-applied force to control jaw opening and closing
- Tip design: Varies based on tissue interaction, including atraumatic, traumatic, and fenestrated configurations
These instruments differ from open surgical forceps by their extended shaft and trocar-based access, which changes how force is applied and perceived during tissue manipulation.
Knowing how the instrument is designed helps clarify why it is widely used in minimally invasive settings.
Why Are Laparoscopic Graspers Important in Minimally Invasive Surgery?
Proper grasper selection enables surgeons to maintain clear visualization of the surgical field by safely retracting organs and tissue away from the operative site. Without appropriate grasping instruments, surgeons face multiple challenges:
- Tissue slippage during critical dissection
- Inadequate retraction obscuring the operative field
- Excessive force application due to poor grip
- Inability to access deep surgical sites safely
These challenges lead directly to iatrogenic injuries if not addressed. The right grasper prevents complications such as bowel perforation, tissue tears, and crush injuries, all of which can extend hospital stays and compromise outcomes.
The same principle of controlled tissue handling continues into the closure phase, where consistent approximation supports healing outcomes.
In minimally invasive procedures, subcutaneous, bioabsorbable systems such as SubQ It! SU-10 helps maintain this consistency for small incisions without the need for external staple placement.
Their clinical value becomes clearer when considering the range of laparoscopic grasper types designed for specific tasks.
6 Key Types of Laparoscopic Graspers
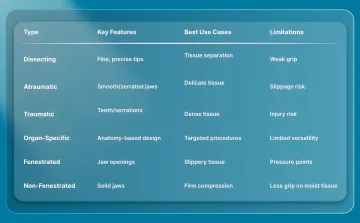
Laparoscopic graspers vary based on jaw design, tissue interaction, and surgical function. Selecting the appropriate type allows surgeons to maintain control while minimizing tissue trauma.
1. Dissecting Graspers
Dissecting graspers are designed for precise tissue separation and blunt dissection, using fine, curved, or pointed tips to identify and develop tissue planes.
Key types and differences:
- Maryland forceps: Curved, fine jaws used for controlled dissection and tissue handling
- Right-angle/Mixter forceps: Angled tip for passing behind vessels and working in confined spaces
- Dolphin/Bullet nose forceps: Rounded tips designed for gentle tissue separation
Best suited for:
- Dissecting tissue planes and identifying anatomical layers
- Isolating vessels and ducts during careful dissection
- Separating adhesions without tearing tissue
- Working in confined spaces where precision matters more than grip strength
Limitations: Dissecting graspers provide limited grip strength and are not suitable for sustained retraction or handling slippery structures.
2. Atraumatic Graspers
Atraumatic graspers are designed with smooth or finely serrated jaws to handle delicate tissue while minimizing compression injury and surface trauma.
Key types and differences:
- Blunt graspers: Smooth jaws for general soft tissue handling
- DeBakey forceps: Fine longitudinal serrations for vascular and delicate tissue
- Duckbill/Fundus graspers: Broad jaws for organ manipulation
- Bowel graspers: Fenestrated jaws designed for intestinal handling
Best suited for:
- Bowel manipulation during gastrointestinal procedures
- Handling delicate organs such as the liver and spleen
- Working with vascular structures requires a controlled grip
Limitations: Atraumatic graspers may lose grip on thick, fibrotic, or high-tension tissue, particularly in moist operative conditions.
3. Traumatic Graspers
Traumatic graspers use teeth or serrations to provide a secure grip on dense or resistant tissue where strong traction is required.
Key types and differences:
- Allis forceps: Interlocking teeth for secure fascial grip
- Babcock forceps: Fenestrated jaws designed for grasping tubular structures with moderate pressure
- Tenaculum forceps: Sharp tips for firm fixation in specific applications
- Rat-tooth forceps: Toothed jaws for a penetrating grip
- Claw forceps: Multiple teeth for maximum tissue purchase
Best suited for:
- Grasping fascia during abdominal wall procedures
- Securing tissue for traction during dissection
- Manipulating fibrotic or scarred tissue
Limitations: Traumatic graspers can cause tissue injury and should not be used on delicate structures such as bowel or vessels.
4. Specialized Organ-Specific Graspers
Specialized graspers are designed with anatomy-specific jaw configurations to optimize control and reduce risk during targeted procedures.
Key types and differences:
- Gallbladder graspers: Fenestrated jaws designed for secure fundus traction
- Appendix graspers: Cupped or fenestrated jaws for tubular structures
- Alligator/Crocodile forceps: Serrated jaws for grasping thicker tissue bundles
Best suited for:
- Gallbladder manipulation during cholecystectomy
- Appendix handling during appendectomy
- Omental or mesenteric tissue manipulation
Limitations: These instruments are optimized for specific tasks and may cause tissue injury if used outside their intended application.
5. Fenestrated vs Non-Fenestrated Graspers
Fenestration refers to openings in the jaws that alter tissue interaction by allowing tissue to sit partially within the jaws rather than relying solely on surface compression.
Key types and differences:
- Fenestrated graspers: Include jaw openings that allow partial tissue enclosure, improving grip on soft or slippery structures
- Non-fenestrated graspers: Use continuous jaw surfaces with serration or texture to apply direct compression for tissue control
Best suited for:
- Fenestrated designs for bowel, mesentery, and other delicate or mobile tissue where slippage is a concern
- Non-fenestrated designs for fascia, fibrotic tissue, and structures requiring firm compression
Limitations: Fenestrated jaws can create localized pressure at window edges if not positioned carefully.
6. Handle Types and Locking Mechanisms
Handle design and locking systems influence force transmission, control precision, and how long tissue can be maintained during laparoscopic procedures.
Key types and differences:
- Pistol-grip handles: Perpendicular design that provides intuitive control and mechanical advantage in force application
- Axial (in-line) handles: Parallel design that aligns with the shaft and may reduce strain in certain working angles
- Ratchet locks: Provide fixed locking positions for sustained tissue retraction
- Slide locks: Allow continuous adjustment based on tissue thickness and required tension
Best suited for:
- Pistol-grip handles for short, controlled maneuvers requiring precision
- Axial handles for prolonged use or specific ergonomic positioning
- Ratchet locks for maintaining consistent retraction
- Slide locks for variable tissue thickness and frequent adjustments
Limitations: Poor handle selection can increase hand fatigue and reduce precision during longer procedures
Each type of laparoscopic grasper serves a specific purpose, which makes the selection process clinically significant.
How to Choose the Right Laparoscopic Grasper in 2026?

Choosing the right laparoscopic grasper directly affects tissue handling, visualization, and the risk of intraoperative injury.
In minimally invasive surgery, where tactile feedback is limited, instrument selection becomes a critical factor in maintaining control and preserving tissue integrity.
1. Assess Tissue Characteristics First
Evaluate tissue properties to match instrument design with tissue behavior and reduce the risk of injury.
- Tissue delicacy: Bowel and vessels require atraumatic graspers, while fascia can tolerate traumatic designs, and solid organs like the liver and spleen benefit from broad, smooth jaws
- Tissue thickness: Thin tissue requires fine tips for precision, while thicker tissue requires stronger jaws for a secure grip
- Tissue moisture/slipperiness: Fenestrated designs improve grip on slippery structures, while serrated or textured jaws are more effective for drier tissue
2. Evaluate Access and Ergonomics
Instrument design must align with access angles and surgeon ergonomics to maintain precision throughout the procedure.
- Port placement: Straight tips for direct access, curved tips for working around structures
- Duration of hold: Locking mechanisms are useful for prolonged retraction, while non-locking designs allow frequent repositioning
- Surgeon preference: Handle type, grip comfort, and instrument weight should match the surgeon's ergonomics
3. Match Instrument to Surgical Phase
Most procedures require multiple graspers, and selecting the right instrument for each phase improves efficiency and safety.
- Initial dissection: Dissecting graspers for tissue plane development
- Organ manipulation: Atraumatic graspers for safe handling
- Fascial work: Traumatic graspers for secure traction
Instrument changes are a routine part of laparoscopic workflows, and efficient selection can reduce unnecessary exchanges and maintain procedural flow.
Final Thoughts
Instrument selection influences outcomes beyond the immediate procedure, particularly in minimally invasive settings where consistency and precision are essential. Standardized tissue handling and closure techniques help reduce variability and support predictable healing.
In this context, SubQ It! SU-10 provides a bioabsorbable subcutaneous closure system for small and laparoscopic incisions. The device places fasteners beneath the skin to achieve precise edge approximation without external staples.
Because the fasteners are absorbable and positioned subcutaneously, no follow-up visit is required for removal.
Contact us to learn how SubQ It! SU-10 can support efficient closure and improved cosmetic outcomes in minimally invasive procedures.
FAQs
1. What are the different types of laparoscopic graspers?
Main categories include dissecting graspers (Maryland, right-angle), atraumatic graspers (blunt, DeBakey, Babcock, bowel), traumatic graspers (Allis, rat-tooth, tenaculum), and organ-specific graspers. Selection depends on tissue type and procedural requirements.
2. What is a laparoscopic grasper used for?
Laparoscopic graspers are used to grasp, hold, manipulate, and retract tissue during minimally invasive procedures, helping maintain visualization and enable precise dissection.
3. What is a fenestrated grasper used for?
Fenestrated graspers have jaw openings that allow tissue to sit within the jaws, improving grip on slippery structures such as bowel while maintaining controlled compression.
4. What is the difference between atraumatic and traumatic graspers?
Atraumatic graspers have smooth or fine serrations for handling delicate tissue such as bowel and vessels, while traumatic graspers have teeth or deep serrations for a strong grip on fascia and dense tissue, and should generally be avoided for delicate structures.
5. How do I prevent tissue damage when using laparoscopic graspers?
Use atraumatic graspers for delicate tissue, apply minimal closing force, and avoid prolonged compression, as limited tactile feedback makes it difficult to detect tissue blanching or deformation.
6. What handle type is best for laparoscopic grasping instruments?
Handle selection depends on surgeon preference and procedural needs, with pistol-grip handles offering mechanical advantage for precision and axial handles supporting ergonomic positioning during prolonged use, both available with ratchet or slide-locking mechanisms for controlled retraction.