Laparoscopic staplers play a central role in minimally invasive surgery, where surgeons need controlled tissue division, reliable access, and consistent staple-line formation through small incisions.
Reports show that the surgical staplers market is expected to reach USD 9.55 billion by 2033, reflecting broader demand for stapling systems across surgical settings.
In laparoscopic cases, small differences in reload selection, jaw positioning, articulation, and firing control can affect the surgeon's efficiency in completing tissue division or anastomosis.
In this blog, you’ll explore how laparoscopic staplers meet surgeon needs in 2026, including device types, reload selection, technique considerations, and workflow impact.
Key Takeaways:
- Laparoscopic staplers help surgeons cut, staple, and approximate tissue through small incisions during minimally invasive procedures.
- Device selection depends on tissue thickness, anatomy, access, reload compatibility, and the surgical goal.
- Linear, powered, circular, reloadable, and single-use staplers serve different procedural needs.
- Proper tissue positioning, compression, firing technique, and staple-line inspection affect stapler performance.
- Internal stapling and external skin closure are separate steps, each requiring the right closure method.
What Is a Laparoscopic Surgical Stapler?
A laparoscopic surgical stapler is an endoscopic instrument used to cut and staple tissue during minimally invasive procedures, enabling controlled tissue division and approximation.
These devices are commonly introduced through trocar ports, most often 12 mm in size, depending on the stapler system and procedure requirements.
Laparoscopic staplers allow surgeons to perform tissue transection, resection, and anastomosis within the confined working space of minimally invasive surgery. This is where access, visualization, and instrument control are more limited than in open procedures.
The distinction is important to understand how laparoscopic staplers differ from other surgical closure and stapling methods.
Key Distinctions
Laparoscopic staplers are used for internal tissue management, not external skin closure. They differ from:
- Skin staplers, which are used for external wound closure
- Open surgical staplers, which require larger access incisions
- Suturing techniques, which rely on manual needle placement and knot tying
In laparoscopic procedures, staplers are primarily used for controlled tissue division with simultaneous staple-line formation and hemostasis.
They are most relevant in situations where manual suturing would increase operative time, reduce consistency, or be technically difficult within a confined laparoscopic field.
Defining what a laparoscopic surgical stapler is also helps clarify the specific surgical needs it is designed to address.
Where Do Laparoscopic Surgical Staplers Meet Surgeon Needs?
 Laparoscopic stapler use is guided by the procedural demands surgeons face during minimally invasive surgery.
Laparoscopic stapler use is guided by the procedural demands surgeons face during minimally invasive surgery.
The device must support controlled tissue division, access in confined anatomy, and consistent staple-line formation without increasing technical complexity.
The following use cases highlight how laparoscopic staplers address specific surgical needs.
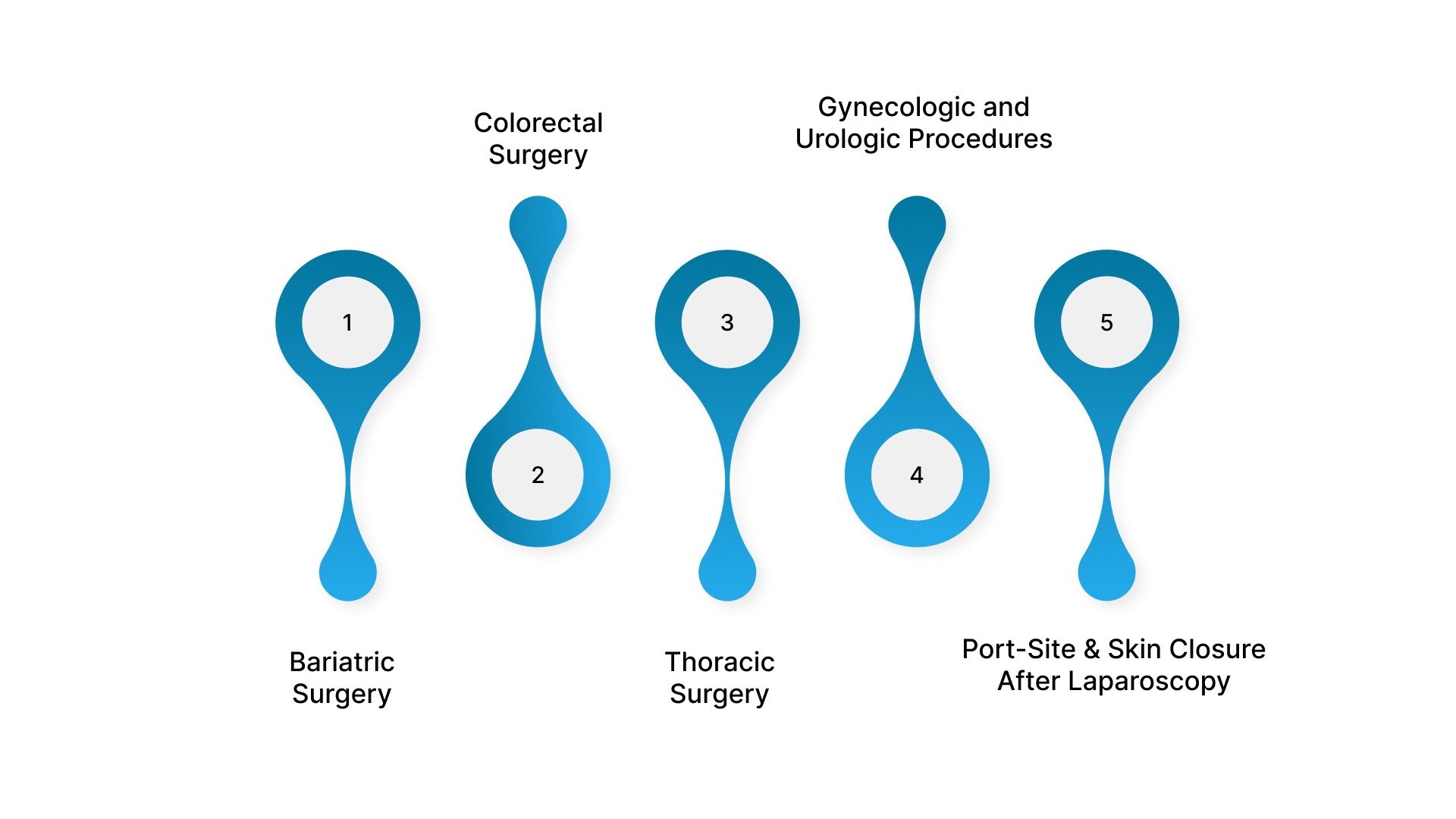
1. Bariatric Surgery
Bariatric procedures require long, continuous staple lines across gastric tissue. Staplers are used to support consistent tissue division and staple-line formation in procedures where precision and repeatability are important.
- Used in sleeve gastrectomy and gastric bypass procedures.
- Supports gastric tissue transection within limited laparoscopic access.
- Requires careful selection of reloads based on tissue thickness and condition.
- Staple-line management may include reinforcement or surgeon-specific technique adjustments.
2. Colorectal Surgery
In colorectal surgery, staplers are used for bowel division and selected anastomoses, particularly in anatomically constrained areas such as the pelvis.
- Used in colectomy and rectal resection procedures.
- Supports bowel transection and anastomosis creation when appropriate.
- Requires accurate tissue positioning before firing, especially in deep pelvic anatomy.
- Post-firing inspection is required to assess staple-line integrity and completeness.
3. Thoracic Surgery
Thoracic procedures require stapling across lung tissue, bronchi, and selected vascular pedicles. Surgeons need devices that allow controlled firing in confined thoracic spaces.
- Used in wedge resection, lobectomy, and lung tissue division.
- Requires device selection based on tissue thickness and anatomical access.
- Articulation may be required for access in limited spaces.
- Inspection is critical for assessing bleeding, air-leak risk, or incomplete staple formation.
4. Gynecologic and Urologic Procedures
In gynecologic and urologic laparoscopy, staplers are used selectively based on procedural need, anatomy, and surgeon preference.
- May be used for tissue division or pedicle control in selected procedures.
- Requires clear visualization before jaw closure and firing.
- Device selection depends on access, tissue type, and procedural indication.
- Should be used only when the device’s function aligns with the surgical objective.
5. Port-Site and Skin Closure After Laparoscopy
Laparoscopic staplers address internal tissue management but do not close the external incision. After trocar removal, surgeons still need a closure method that fits the incision size, cosmetic goals, and follow-up workflow.
- Manual suturing provides control but may increase closure time.
- External metal staples are fast but typically require removal and may leave visible puncture marks.
- For small laparoscopic incisions, this is where a bioabsorbable subcuticular option, such as SubQ It! SU-10 fits naturally, as it places fasteners beneath the skin, eliminating the need for external staple removal.
Understanding the clinical needs these devices address also provides context for how a laparoscopic surgical stapler functions during a procedure.
How Does a Laparoscopic Surgical Stapler Work?
A laparoscopic surgical stapler works by compressing tissue, deploying staples, and, in linear cutting devices, dividing tissue between staple rows.
This coordinated mechanism allows surgeons to perform tissue division and approximation in a single controlled action.
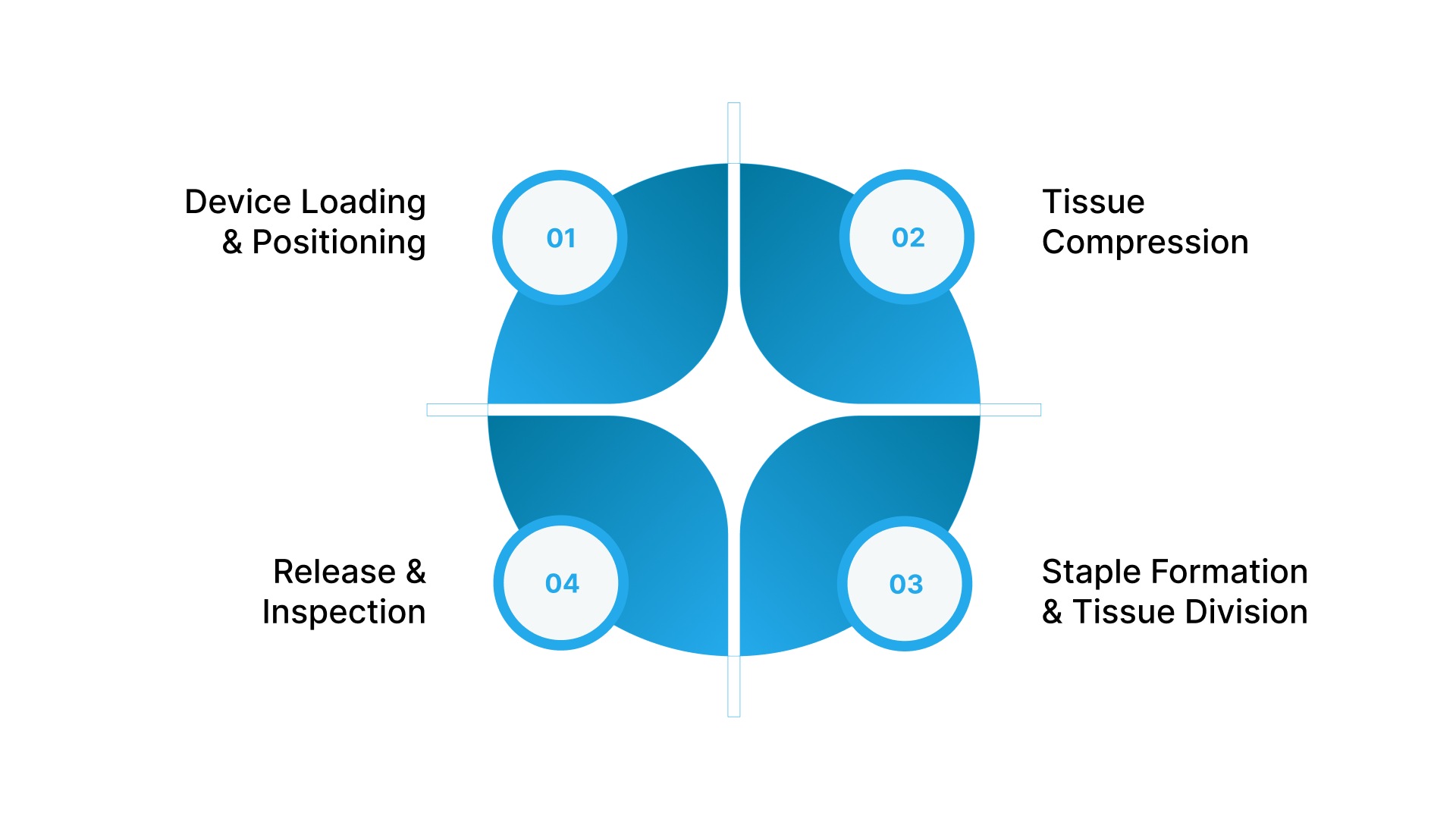
The sequence below outlines the general workflow for endoscopic linear cutting staplers, noting that exact steps may vary by manufacturer and device.
1. Device Loading and Positioning
The process begins with selecting a cartridge or reload that matches the tissue type, tissue thickness, and intended staple line. Most stapling systems include a cartridge, anvil, and firing mechanism that work together during deployment.
- Many systems use color-coded reloads to guide staple height selection, though standards vary by manufacturer.
- Select the reload based on tissue thickness, vascularity, and procedural objective.
- Introduce the stapler through an appropriately sized trocar port.
- Advance the jaws to the target tissue under laparoscopic visualization.
- Position tissue evenly between the cartridge and anvil before closure.
2. Tissue Compression
Closing the stapler jaws brings the cartridge and anvil together, compressing the tissue before firing. This step prepares the tissue for proper staple formation and allows the surgeon to confirm alignment.
- Confirm tissue is not folded, twisted, or unevenly captured.
- Avoid firing across tissue that does not match the selected reload range.
- Follow device-specific guidance for compression rather than applying a fixed timing rule.
- Compression helps optimize staple formation and tissue approximation prior to firing.
3. Staple Formation and Tissue Division
When the stapler is fired, the internal firing mechanism advances through the cartridge. Staples are driven through the tissue and formed against the anvil, while an integrated blade divides tissue between staple rows in linear cutting staplers.
- Staples are typically formed into a B-shaped configuration against the anvil.
- Linear cutting staplers deploy multiple staggered rows of staples on each side of the cut line.
- An integrated blade divides tissue between the staple rows during firing.
- This coordinated action allows simultaneous tissue division and staple-line creation.
4. Release and Inspection
After firing, the surgeon opens the jaws and removes the stapler carefully. The staple line must be inspected before proceeding, as device performance depends on proper technique and tissue conditions.
- Check for complete firing and proper staple formation.
- Inspect for bleeding, tissue disruption, or incomplete division.
- Confirm the tissue was divided as intended.
- Determine whether reinforcement, oversewing, or correction is required.
A clear understanding of how the device works also helps explain the different types of laparoscopic surgical staplers used in practice.
4 Key Types of Laparoscopic Surgical Staplers
Laparoscopic staplers are not interchangeable across procedures. Surgeons select them based on access, tissue characteristics, firing control, anatomy, and the specific surgical objective.
The following categories reflect the main types and configurations used in laparoscopic surgery.
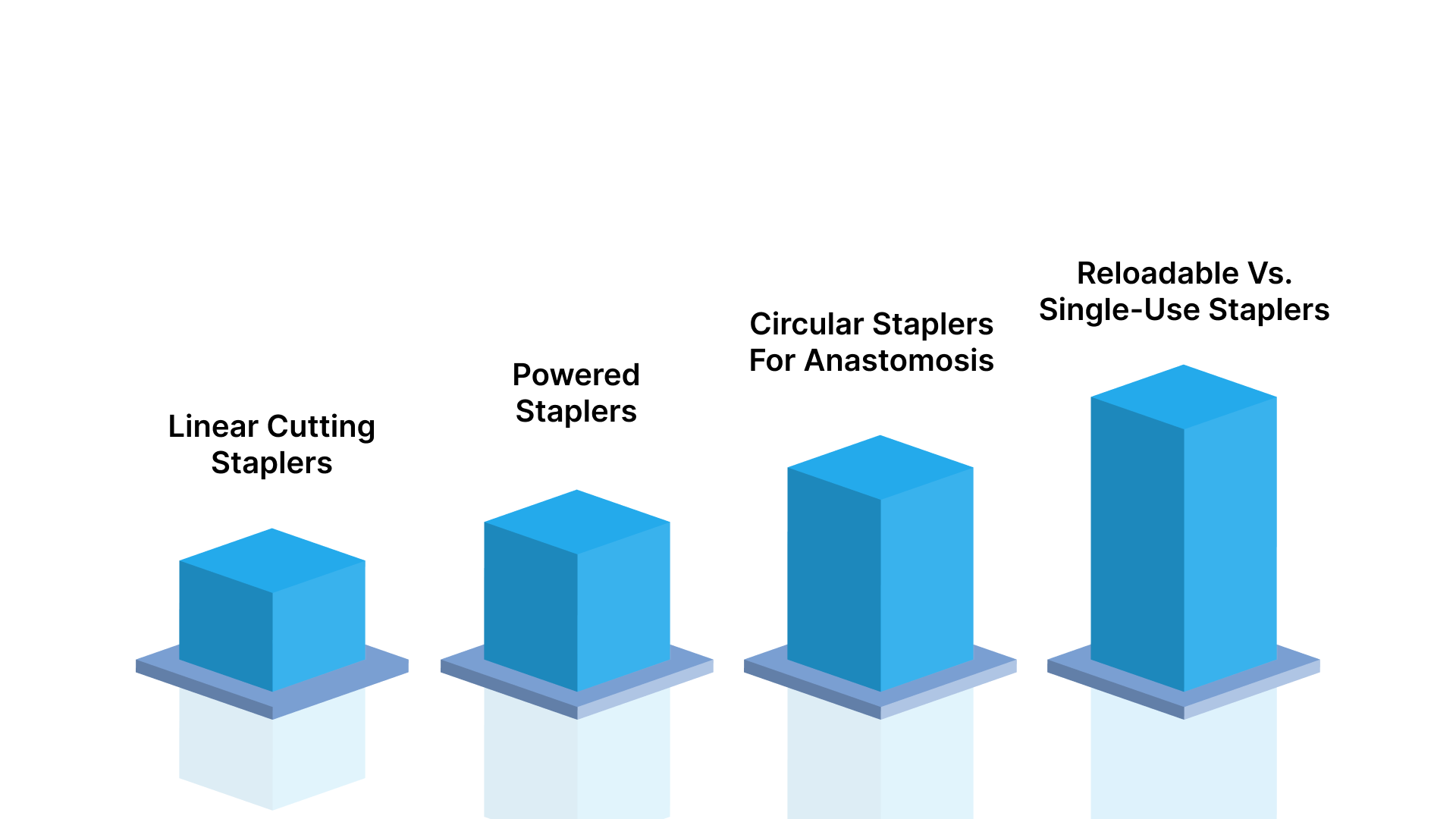
1. Linear Cutting Staplers
Linear cutting staplers, often called endoscopic linear cutters, create a straight staple line and divide tissue between staple rows. They are commonly used when controlled tissue transection or resection is required.
- Used for bowel resection, gastric transection, lung tissue division, and similar internal steps
- Available in different shaft lengths, jaw designs, and reload options depending on the device system.
- May include straight or articulating jaws to improve access in confined laparoscopic anatomy
- Cartridge length and staple height should be selected based on tissue type, thickness, and manufacturer guidance.
2. Powered Staplers
Powered staplers use a motorized firing mechanism rather than relying entirely on manual hand force. This can reduce variability in firing, particularly in difficult angles or longer procedures.
- May support more consistent firing speed and compression compared to manual systems
- Can be useful in deep pelvic, thoracic, or bariatric procedures where control is critical
- May reduce user-dependent variation during firing
- Still requires correct reload selection, tissue positioning, and staple-line inspection.
3. Circular Staplers for Anastomosis
Circular staplers are used to create anastomoses between hollow structures, most commonly in colorectal and upper gastrointestinal procedures.
- Used for end-to-end or end-to-side anastomoses
- Require correct anvil placement and alignment with the stapler body
- Create a circular staple line while removing a tissue “donut.”
- The surgeon must inspect tissue donuts after firing to confirm completeness.
4. Reloadable vs. Single-Use Staplers
Laparoscopic stapling systems may use reusable handles with disposable reloads, fully disposable devices, or platform-specific configurations. Selection depends on procedural needs, workflow, and institutional protocols.
- Reloadable systems allow multiple cartridge uses with a single handle during a procedure.
- Single-use systems reduce reprocessing steps and simplify device management.
- Cartridge compatibility and availability affect intraoperative workflow
- Cost considerations should include device use, reload consumption, and procedural efficiency
Reviewing the different types also provides helpful context before outlining the key considerations for selecting laparoscopic staplers.
5 Key Considerations for Selecting Laparoscopic Staplers
Selecting a laparoscopic stapler is a clinical decision that depends on tissue characteristics, anatomy, procedural goals, and intraoperative workflow. The stapler, reload, and firing technique must align with these factors to support safe and consistent staple-line formation.
The following considerations guide device selection in laparoscopic surgery.
1. Matching Staple Height to Tissue Characteristics
Staple height must match the target tissue's compressed thickness and condition. Incorrect selection can affect staple formation, tissue perfusion, and staple-line integrity.
- Assess tissue thickness before selecting a reload.
- Consider vascularity, edema, inflammation, fibrosis, and tissue fragility.
- Use manufacturer guidance for cartridge selection.
- Avoid firing across tissue that does not fall within the recommended compression range.
- Reassess if tissue appears unusually thick, friable, or unevenly captured.
2. Technique and Operator Factors
Stapler performance depends on surgeon technique as much as device selection. Tissue handling, compression, and inspection directly influence staple-line quality.
- Position tissue evenly between the cartridge and anvil.
- Avoid excessive traction or tissue distortion before firing.
- Follow device-specific instructions for compression and firing.
- Confirm that unintended structures are not captured.
- Inspect the staple line after firing for bleeding, incomplete formation, or disruption.
3. Access and Maneuverability
Laparoscopic stapling occurs in confined spaces with limited angles. Device design must support safe positioning without compromising visualization or tissue handling.
- Consider shaft length, jaw length, and articulation requirements.
- Use articulating staplers when straight-line access is limited.
- Select devices that can be introduced through planned trocar sizes.
- Avoid forcing device placement in restricted anatomy.
- Match device configuration to procedural access requirements.
4. Balancing Cost with Clinical Use
Device selection should reflect procedural needs rather than cost alone. In complex cases, device capabilities may be more important than upfront price.
- Match the stapler features to the procedure rather than defaulting to advanced options.
- Consider reload usage, inventory, and team familiarity.
- Evaluate whether powered or articulating systems add value in that case.
- Avoid selecting a device based only on cost when anatomy or tissue complexity is high.
- Consider overall workflow efficiency, not just device price.
5. Closure Needs After Laparoscopic Stapling
Laparoscopic staplers manage internal tissue but do not address skin closure. After trocar removal, surgeons must select a closure method that fits the incision size, cosmetic expectations, and follow-up requirements.
- Traditional metal staples are fast but require removal and may leave visible puncture marks.
- Manual suturing provides controlled approximation but may increase closure time.
- Bioabsorbable subcuticular systems are designed to place staples under the skin without piercing the outer surface.
- These systems eliminate the need for staple removal and support a different closure workflow compared to external staples.
Final Thoughts
Choosing the right laparoscopic stapler affects internal tissue control, staple-line consistency, and overall procedural flow.
Once the laparoscopic work is complete, skin closure becomes the next point where speed, cosmetic expectations, and follow-up requirements matter.
In this context, SubQ It! SU-10 offers a bioabsorbable subcuticular closure system for small and laparoscopic incisions up to 10 cm. It places fasteners beneath the skin, so there is no external staple removal step.
Contact us today to explore how SubQ It! SU-10 can support laparoscopic port-site closure and closure workflow.
FAQs
1. What is a laparoscopic stapler used for?
Laparoscopic staplers are used to cut and staple tissue during minimally invasive surgery, supporting resection, vessel control, and anastomosis creation. They allow surgeons to perform these steps through small incisions while achieving tissue approximation and hemostasis.
2. What kind of staples are used in laparoscopic surgery?
Most laparoscopic staplers use metal staples (commonly titanium or stainless steel) that deform into a B-shaped configuration when fired. This shape helps compress and secure tissue while maintaining blood flow at the staple line.
3. What is the difference between linear and circular laparoscopic staplers?
Linear staplers create straight staple lines and divide tissue, while circular staplers are used to create anastomoses between tubular structures. The choice depends on whether the surgical goal is tissue division or reconnection.
4. How do surgeons choose the right staple cartridge size?
Surgeons select cartridge size based on tissue thickness, condition, and intraoperative assessment, following manufacturer guidance. Incorrect selection can affect staple formation and compromise tissue integrity.
5. What are the common complications associated with laparoscopic stapler use?
Complications are typically related to tissue selection, compression, or technique, rather than device failure. These may include staple-line leaks, bleeding, or staple malformation.
6. Can laparoscopic staplers be used on all tissue types?
No, laparoscopic staplers are not suitable for all tissues, especially those that are too thick, calcified, or too fragile to compress properly. Surgeons must confirm the tissue falls within the device’s recommended range before firing.
7. What is the basic anatomy of a surgical stapler?
A surgical stapler typically consists of a handle (actuation mechanism), shaft, cartridge containing staples, an anvil for staple formation, and a firing mechanism that drives the staples through tissue.