Staple line integrity plays a central role in the progression of a procedure, particularly in gastrointestinal, thoracic, and bariatric surgery, where bleeding or seal failure may relate to device selection and tissue handling.
As the use of stapling systems expands, the U.S. surgical staplers market is projected to reach USD 4 billion by 2034, reflecting growing procedural reliance.
In high-volume operating rooms, linear staplers help standardize transection and closure; however, their performance varies with staple height, articulation, and firing mechanism.
In this blog, you will learn what surgeons should know about linear staplers, including how they work, their types and designs, key features, surgical uses, and selection considerations.
Key Takeaways:
- Linear staplers place staggered rows of staples and can cut tissue, supporting controlled transection and hemostasis.
- Non-cutting staplers are used for tissue approximation, while cutting staplers combine sealing and division in one step.
- Laparoscopic staplers provide reach and articulation for confined spaces, while open staplers allow direct positioning and larger tissue handling.
- Proper compression, alignment, and cartridge selection are critical; errors increase the risk of leaks, bleeding, or staple line failure.
- Staple height, jaw length, articulation, firing mechanism, and compression control determine consistency and intraoperative efficiency.
What Is a Linear Stapler in Surgery?
A linear stapler is a surgical device that places one or more staggered rows of staples in a straight line to approximate tissue and achieve hemostasis. In variants with an integrated blade (linear cutter staplers), it can simultaneously divide tissue during transection.
It is widely used in gastrointestinal, thoracic, and bariatric surgery, particularly where consistent staple line formation is required.
Once the function is outlined, the differences in device design become more relevant.
Key Types of Linear Stapler Devices
Linear staplers are most commonly classified based on their functional role during surgery, which determines whether they are used for tissue approximation alone or for combined transection and closure.
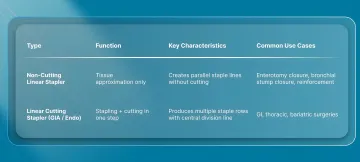
1. Linear Stapler (Non-Cutting)
A non-cutting linear stapler places rows of staples without dividing tissue. It is used when tissue approximation, reinforcement, or closure is required without transection.
Key characteristics include:
- Creates parallel staple lines without cutting
- Used for closure of enterotomies, bronchial stumps, or tissue reinforcement
- Applied selectively depending on the procedural step
2. Linear Cutting Stapler (Endo Linear Stapler / GIA)
A linear cutting stapler simultaneously places multiple staggered rows of staples and divides tissue in a single firing sequence.
Key characteristics include:
- Combines stapling and cutting in one step
- Produces multiple staple rows with a central division line
- Widely used in gastrointestinal, thoracic, and bariatric surgery
Beyond core device types, linear staplers are also differentiated by surgical access requirements.
What Are the Different Linear Stapler Designs Based on Surgical Access?
Linear staplers are commonly classified based on how they are introduced into the surgical field, which directly affects access, control, and maneuverability.
1. Laparoscopic Linear Stapler
It is designed for minimally invasive surgery through trocar ports. This type of stapler prioritizes reach and precision in confined spaces.
Key characteristics:
- Compatible with laparoscopic ports
- Long shaft for deep anatomical access
- Articulation for difficult angles
- Used in laparoscopic GI, bariatric, and thoracic (VATS) procedures
2. Open Linear Stapler
It is used in open surgery with direct access to the operative field, allowing simpler positioning and broader tissue engagement.
Key characteristics:
- Larger jaw lengths
- No port or shaft constraints
- Direct manual positioning with full visualization
- Used in open gastrointestinal, thoracic, and general surgery
For procedures involving longer incisions, SubQ It! SU-25 can be used during skin closure, providing a bioabsorbable subcutaneous approach that maintains procedural efficiency without removal.
Once the design variations are clear, understanding the mechanism behind their function becomes equally important.
How Does a Linear Stapler Work?
A linear stapler functions through a coordinated sequence of tissue compression, staple formation, and optional division, all of which determine staple line integrity and complication risk.
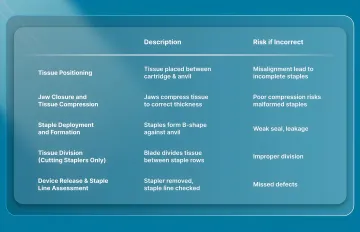
Here’s how a linear stapler works:
1. Tissue Positioning
The target tissue is placed between the cartridge and anvil with proper alignment before firing.
- Tissue must sit evenly within the jaws
- Misalignment can lead to incomplete staple formation
- Adequate exposure is required before closure
2. Jaw Closure and Tissue Compression
The jaws are closed to apply uniform compression, reducing tissue thickness to match the selected cartridge.
- Compression is essential for proper staple formation
- Cartridge selection must match tissue thickness
- Inadequate compression increases the risk of malformed staples
3. Staple Deployment and Formation
On firing, staples are driven through tissue and formed against the anvil into a B-shape.
- Multiple staggered rows improve strength and seal integrity
- B-shaped staples secure tissue while maintaining perfusion
- Formation depends on correct compression and cartridge choice
4. Tissue Division (Cutting Staplers Only)
In linear cutting staplers, a blade advances between staple rows during firing.
- The central blade divides the tissue between the sealed edges
- Enables simultaneous transection and closure
5. Device Release and Staple Line Assessment
After firing, the stapler is opened and removed, leaving a sealed staple line.
- The staple line should be uniform and intact
- No gaps or malformed staples should be present
- Final inspection is required before proceeding
Once the operational process is clear, it becomes easier to identify the features that influence performance.
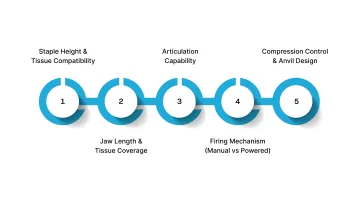
5 Key Features to Evaluate in a Linear Stapler
Selecting a linear stapler requires assessing features that directly influence staple formation, tissue perfusion, and intraoperative efficiency.
These factors determine how reliably the device performs across different tissue types and procedural steps.
1. Staple Height and Tissue Compatibility
Staple height must match the thickness of compressed tissue, as a mismatch is a primary driver of staple-line failure and complications.
- Too high: Inadequate tissue apposition, increased risk of leak or bleeding
- Too low: Excessive compression, risk of ischemia and tissue injury
Tissue characteristics (edema, fat, fibrosis) can alter effective thickness intraoperatively. In addition, cartridge selection must align with manufacturer-defined thickness ranges
2. Jaw Length and Tissue Coverage
Jaw length determines how much tissue can be captured in a single firing and how many firings are required to complete the transection or closure.
- 30 mm: Confined or narrow operative fields
- 45–60 mm: Standard laparoscopic applications
- 75–100 mm: Open procedures and larger tissue segments
Longer jaws can reduce the number of firings, which:
- Improves procedural efficiency
- Minimizes staple line intersections, a known point of weakness
3. Articulation Capability
Articulation allows the stapler to adjust its angle relative to tissue, improving both access and alignment.
- Typically provides 45° angulation.
- Enables perpendicular alignment to tissue, which is critical for uniform staple formation
- Particularly important in the pelvis, mediastinum, and deep abdominal spaces
4. Firing Mechanism (Manual vs Powered)
The firing mechanism determines how the compression and staple-deployment forces are applied across the tissue.
- Manual: Provides tactile feedback but depends on surgeon-applied force
- Powered: Delivers consistent firing force, reducing variability
Powered systems have been associated with:
- More consistent staple formation
- Reduced variability in thick or fibrotic tissue
- Lower complication rates in some settings
5. Compression Control and Anvil Design
Compression and anvil geometry directly determine how staples are formed and how evenly the force is distributed.
- Uniform pre-firing compression is required for proper staple formation
- Some devices include compression indicators to guide readiness
- The anvil shapes staples into a B-configuration, ensuring secure closure
- Uneven compression can result in malformed staples and weak staple lines
The importance of these features is reflected in the range of procedures where linear staplers are applied.
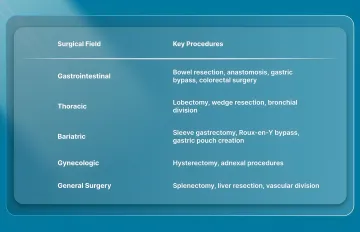
5 Common Surgical Uses of Linear Staplers in 2026
A linear stapler is used in procedures requiring controlled tissue transection, reliable hemostasis, and consistent staple line formation. Its role is defined by the need to standardize critical steps such as division, sealing, and anastomosis.
1. Gastrointestinal Surgery
Linear staplers are widely used in GI surgery for both tissue division and anastomosis creation, where staple-line integrity directly affects the risk of leakage.
- Bowel resection and transection
- Side-to-side intestinal anastomosis
- Gastric bypass (gastrojejunostomy)
- Colorectal resections
They are particularly suited for intracorporeal reconstruction and side-to-side anastomosis techniques.
2. Thoracic Surgery
In thoracic procedures, linear staplers are used for lung parenchymal division and airway control, where secure sealing is required to prevent air leaks.
- Lung wedge resection
- Lobectomy and segmentectomy
- Division of bronchial and pulmonary vascular structures
Staple line quality directly affects air leak rates and postoperative recovery.
3. Bariatric Surgery
Bariatric procedures rely heavily on linear staplers for gastric division and reconstruction, where long staple lines must remain secure under pressure.
- Sleeve gastrectomy
- Roux-en-Y gastric bypass
- Gastric pouch formation
Staplers are essential for creating uniform, leak-resistant staple lines in gastric tissue.
4. Gynecologic Surgery
Linear staplers are used selectively in gynecologic procedures, particularly in advanced laparoscopic or oncologic settings requiring controlled transection.
- Hysterectomy (selected cases)
- Ovarian and adnexal procedures
Their use depends on surgeon preference and procedural complexity.
5. General and Other Surgical Applications
Linear staplers are also used in procedures involving solid organ transection and vascular control, where consistent closure is required across variable tissue types.
- Splenectomy
- Liver resection
- Division of the mesentery and vascular pedicles
These applications rely on reliable hemostasis and rapid tissue division.
As linear staplers support multiple operative applications, the decision-making process for selecting the right one is clinically significant.
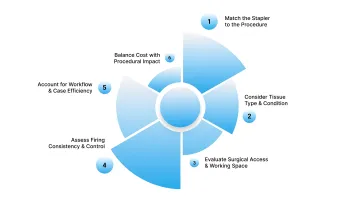
How to Choose the Right Linear Stapler?
Choosing a linear stapler requires aligning the device with the specific procedure, tissue type, and surgical environment to ensure consistent and reliable staple formation.
Surgeons should evaluate the following key factors:
1. Match the Stapler to the Procedure
The first consideration is whether the surgery requires tissue transection, anastomosis, or reinforcement. Cutting staplers allow simultaneous division and closure, while non-cutting staplers are used for reinforcement or tissue approximation.
2. Consider Tissue Type and Condition
Fragile tissue, such as bowel or lung tissue, requires controlled compression, whereas thick or fibrotic tissue requires a higher staple height.
Edematous or inflamed tissue increases the risk of staple line failure if mismatched. Staple height must match the thickness of the compressed tissue to ensure proper formation.
3. Evaluate Surgical Access and Working Space
The operative field determines how easily the stapler can be positioned and fired. Confined or deep spaces, such as the pelvis or mediastinum, require articulating staplers for precise placement.
Laparoscopic procedures require adequate shaft length and controlled angulation. Open procedures allow larger jaws and direct control, but still require proper alignment for consistent staple formation.
4. Assess Firing Consistency and Control
Consistent firing reduces variability in staple formation, which is critical for hemostasis and leak prevention. Powered staplers offer more uniform force across the staple line, while manual staplers rely on surgeon-applied pressure.
5. Account for Workflow and Case Efficiency
Device selection impacts operative time and overall workflow. Staplers that require fewer reloads or allow smooth articulation reduce interruptions during surgery.
Reducing the number of firings also minimizes staple line intersections, which are potential weak points.
6. Balance Cost with Procedural Impact
Cost evaluation should consider total procedural efficiency and patient outcomes, not just per-unit price. Higher-cost devices may reduce operative time or complication rates, offsetting upfront expenses.
Surgeons should weigh the impact on OR time, potential complications, and case volume when selecting a stapler.
Final Thoughts
Staple line formation does not end with successful transection or anastomosis. It continues to influence tissue healing, the management of complications, and the consistency of outcomes across different procedures.
As expectations for precision and efficiency increase, attention is shifting toward how closure methods support the entire surgical workflow.
In this setting, SubQ It! SU-25 supports longer incisions with a subcutaneous, device-assisted approach. Its handheld system places bioabsorbable dermal fasteners beneath the skin without external penetration, saving approximately 25 minutes per case.
Contact us today to explore how SubQ It! SU-25 fits into your surgical workflow, and learn more about this advanced system.
FAQs
1. What is the difference between linear and circular staplers?
Linear staplers create straight staple lines for transection and side-to-side anastomoses, often cutting and stapling simultaneously. Circular staplers create end-to-end or end-to-side anastomoses in tubular structures and include a circular blade that excises tissue during firing.
2. How to select the correct staple height based on tissue thickness?
Choose the staple height based on the compressed thickness and tissue characteristics, as each cartridge delivers a specific closed staple height that determines the level of tissue compression.
3. What are the most common complications associated with linear staplers?
Common complications include anastomotic leaks, bleeding, staple line failure, and tissue ischemia. These are typically linked to improper staple height selection, inadequate compression, or device misfiring.
4. Should you choose a powered or manual linear stapler?
Powered staplers provide consistent firing and reduce fatigue, while manual staplers offer tactile feedback at a lower cost. Powered devices may reduce variability and complications in some procedures, though outcomes vary by context.
5. How do articulating linear staplers improve surgical outcomes?
Articulation about 45° improves access in confined spaces, such as the pelvis or mediastinum. It enables more precise positioning and controlled staple-line placement.
6. What factors should be checked before firing a linear stapler?
Ensure proper tissue alignment, adequate compression, and correct cartridge selection before firing. Misalignment or insufficient compression can result in malformed staples, bleeding, or anastomotic failure.