Securing vessels and ducts is a routine yet critical step that shapes operative flow, particularly in minimally invasive surgery, where space and instrument control are limited. In these settings, efficient ligation supports both procedural speed and consistency.
With more than 15 million procedures annually in the United States involving ligation devices, their role across specialties is well-established.
Ligation clips provide rapid occlusion without intracorporeal suturing, though performance varies by material and design.
In this blog, you’ll learn what ligation clips are, the different types and materials available, their clinical uses, safety considerations, and how to select the right clip in practice.
Key Takeaways:
- Ligation clips provide faster, more consistent vessel and duct occlusion than manual suturing, especially in laparoscopic procedures.
- Clips are made of titanium, non-absorbable polymer, or absorbable polymer, each affecting permanence, imaging, and conductivity.
- Clip selection should consider vessel diameter, wall thickness, location, and procedure requirements to ensure secure occlusion.
- Absorbable clips lower the risk of complications such as bile leakage and reduce the long-term presence of foreign material in the body.
- Using clips consistently improves surgical workflow, reduces variability, and enhances efficiency in high-volume or confined procedures.
What Are Ligation Clips and Why Are They Important?
Ligation clips are small mechanical devices applied to blood vessels or tubular structures such as ducts, arteries, or fallopian tubes to stop blood flow or close luminal structures.
They function by mechanically compressing tissue, creating a seal that prevents bleeding or fluid passage.
Compared to manual suture ligation, clip application generally reduces the time required for vessel occlusion, particularly in laparoscopic procedures.
In laparoscopic cholecystectomy, clips are routinely used to secure the cystic duct and artery, reflecting their widespread adoption in minimally invasive surgery.
Why ligation clips matter in surgical practice:
- Speed: Clip application typically requires less time than intracorporeal suture ligation for vessel occlusion
- Access: Enables vessel control in confined laparoscopic environments where suturing is technically complex
- Hemostasis: Provides immediate mechanical occlusion of vessels and ducts
- Consistency: Standardized application reduces variability compared to manual knot tying
Once their importance is clear, it becomes useful to review the main types used in practice.
3 Key Types of Ligation Clips in Surgery
Ligation clips differ in material, size, and locking mechanism, and these characteristics determine their suitability for specific vessel sizes and surgical applications.
In practice, clip selection is driven by tissue characteristics, required occlusion strength, and intraoperative workflow considerations.
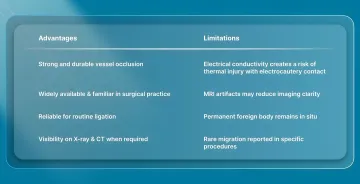
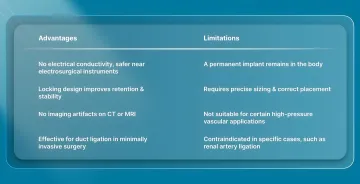
1. Metal Titanium Ligation Clips
Titanium clips are widely used in open and laparoscopic procedures due to familiarity and consistent mechanical performance.
Key considerations:
- Titanium clips remain permanently in the body and do not degrade after placement.
- Radiopaque structure allows identification on X-ray and CT imaging.
- MRI compatibility is maintained, but imaging artifacts can obscure adjacent structures.
- Compression strength supports occluding small- to medium-sized vessels in routine surgical use.
Advantages and Limitations:
2. Non-Absorbable Polymer Ligation Clips
Polymer clips are used to improve retention and eliminate conductivity risks, particularly in laparoscopic procedures.
Key considerations:
- Non-conductive material prevents unintended energy transmission during electrosurgery.
- Integrated locking mechanisms improve grip and reduce the risk of slippage after deployment.
- Radiolucent composition avoids artifacts on CT and MRI imaging.
- Frequent use in duct ligation during laparoscopic procedures such as cholecystectomy.
Advantages and Limitations:
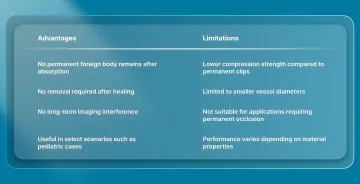
3. Absorbable Polymer Ligation Clips
Absorbable clips provide temporary occlusion and degrade after the healing phase.
Key considerations:
- Bioabsorbable polymers break down over time after fulfilling the occlusion function.
- Mechanical support is maintained during the early healing phase before gradual absorption.
- No permanent implant remains after degradation.
- Use is limited to smaller vessels and cases where long-term foreign material is not preferred.
Advantages and Limitations:
Beyond their design differences, their value becomes clearer when viewed in specific clinical applications.
3 Clinical Uses of Ligation Clips in Surgery
Ligation clips are used to achieve rapid mechanical occlusion of vessels and ducts during both open and minimally invasive procedures. Here’s how ligation clips are used across common surgical settings.
1. Laparoscopic and Minimally Invasive Surgery
Ligation clips are widely used in minimally invasive procedures where limited access makes intracorporeal suturing technically demanding. Clip application allows controlled occlusion without knot tying in confined operative fields.
In these settings, absorbable systems, such as SubQ It! SU-25 provide subcutaneous closure for longer incisions, maintaining secure vessel control while eliminating the need for follow-up removal.
- Cholecystectomy: Clips occlude the cystic duct and cystic artery prior to division.
- Appendectomy: Clips control mesoappendix vessels and, in selected cases, secure the appendiceal stump.
- Gynecologic Procedures: Clips are applied for tubal occlusion and control of ovarian or uterine vessels.
- Bariatric Procedures: Clips control small gastric vessels during dissection in procedures such as sleeve gastrectomy or bypass.
2. Open Surgical Procedures
Ligation clips are used in open procedures to rapidly control small and medium-sized vessels during dissection. Clip application reduces the need for repeated suture ligation in areas with multiple small vascular branches.
- Thyroid and Parathyroid Surgery: Clips control small vessels in highly vascular operative fields.
- Vascular Surgery: Clips secure branch vessels during exposure and dissection.
- Oncologic Resections: Clips control tumor-feeding vessels during tissue mobilization.
3. Duct and Tubular Structure Occlusion
Ligation clips are used to occlude ducts and tubular structures where secure closure is required before division. Selection depends on duct diameter and the risk of leakage under physiological pressure.
Proper sizing and placement are required to ensure complete occlusion.
- Biliary Surgery: Clips close the cystic duct before gallbladder removal.
- Gynecologic Surgery: Clips provide permanent tubal occlusion for sterilization procedures.
- Selected Procedures: Clips may be used for vascular or ductal control depending on the surgical approach and anatomy.
While their uses are well established, understanding the associated safety considerations is equally important.
5 Safety Considerations & Potential Complications to Consider in 2026
Ligation clips are widely used in surgical practice and have a well-established safety profile. Complications are uncommon but can occur due to improper application, material properties, or anatomical factors.
1. Mechanical Complications
Mechanical failure is typically related to clip placement, sizing, or tissue characteristics.
- Clip migration: Migration can occur after procedures such as cholecystectomy, in which a clip may enter the common bile duct and serve as a nidus for stone formation.
- Incomplete occlusion: Inadequate closure of a vessel or duct can result in bile leakage or hemorrhage, requiring intervention. Reported bile leak rates after laparoscopic cholecystectomy are approximately 0.4-0.6%.
- Clip dislodgement: Dislodgement is associated with radial shearing forces and improper sizing or placement. Locking or double-shanked clip designs provide greater resistance to displacement compared to simpler designs.
2. MRI Safety and Imaging Considerations
Material selection affects both MRI compatibility and post-operative imaging quality.
- Titanium clips: Non-ferromagnetic and considered MR conditional under standard clinical conditions, but may produce artifacts that obscure adjacent structures.
- Polymer clips: Non-conductive and radiolucent, with no imaging artifacts on CT or MRI.
- Absorbable clips: Contain no metal and do not produce imaging artifacts after placement or degradation.
- Imaging impact: Metal clips can reduce diagnostic clarity in imaging studies by creating localized artifacts near the clip site.
3. Biocompatibility Concerns
Tissue response varies depending on material composition and duration of implantation.
- Allergic reactions: Titanium is generally biocompatible. Rare allergic responses have been reported in patch testing studies, but clinical reactions remain uncommon.
- Tissue inflammation: Permanent clips may be associated with localized chronic inflammation or foreign body granuloma formation in some patients.
4. Electrical Safety During Electrosurgery
Electrical interaction depends on the conductivity of the clip material.
- Metal clips: Conduct electrical current and may transmit energy if contacted by an active electrode, creating a risk of unintended thermal injury.
- Technique consideration: Direct contact between electrosurgical instruments and clips should be avoided.
- Polymer clips: Non-conductive and do not transmit electrical energy, making them suitable when extensive electrocautery is used near clipped structures.
5. Proper Application Technique
Correct technique is essential to minimize mechanical and clinical complications.
- Size selection: Select a clip size appropriate for the vessel diameter to ensure secure occlusion.
- Vessel capture: Ensure complete inclusion of the vessel or duct within the clip jaws before deployment.
- Placement: Avoid positioning clips too close to critical structures such as ducts or nerves.
- Closure verification: Confirm full clip closure before releasing the applicator.
- Tissue considerations: Post-operative tissue changes, including edema reduction, may alter vessel diameter and contribute to clip instability if sizing is inadequate.
Addressing safety considerations also reinforces the importance of selecting the appropriate clip for each procedure.
How to Select the Right Ligation Clip for Your Procedure?
Clip selection depends on vessel characteristics, procedural requirements, and material behavior in the operative field. The following factors guide clip selection in routine surgical practice.
1. Key Selection Criteria
Clip choice must account for anatomical and procedural factors to ensure reliable occlusion of a vessel or duct.
- Vessel diameter and wall thickness: Vessel size and tissue quality determine clip size selection and directly affect retention and occlusion reliability.
- Surgical approach: Laparoscopic procedures require clip systems compatible with minimally invasive applicators, while open procedures allow greater flexibility in instrument choice.
- Permanence requirements: Permanent occlusion requires non-absorbable clips, while absorbable clips are used when temporary support during healing is sufficient.
2. Practical Decision-Making Factors
Selecting the right clip also depends on institutional resources and the surgeon's experience. Practical constraints such as available instruments, cost, and evidence-based outcomes inform the final choice.
- Institutional availability: Clip selection is influenced by formulary restrictions, cost considerations, and available inventory.
- Surgeon familiarity: Familiarity with a specific clip system affects application accuracy and intraoperative efficiency.
- Instrument compatibility: Clip systems must be compatible with existing applicators and laparoscopic setups.
- Clinical evidence: Selection should be informed by procedure-specific outcomes data and established clinical use.
3. Procedure-Specific Considerations
Certain procedures have specific requirements that influence clip choice. Evidence and clinical experience guide safe and effective use for each indication.
- Cystic duct closure: Absorbable clips have been associated with lower bile leakage rates compared to permanent metal clips in some studies, although outcomes vary by technique and patient factors.
- General vessel ligation: Available evidence shows no consistent difference in overall complication rates between polymer and metal clips across most applications.
Final Thoughts
Effective vessel ligation extends beyond simply stopping blood flow. It shapes operative efficiency, procedural consistency, and postoperative outcomes across surgical specialties.
As surgeons manage increasing caseloads, the precision, speed, and reliability of closure devices become essential to workflow and patient safety.
In this setting, SubQ It! SU-25, with 25 staples closing incisions up to 25 cm, provides a subcutaneous, device-assisted solution for longer procedures.
Its handheld system places absorbable fasteners beneath the skin, saves approximately 25 minutes per case, and increases the private clinic surgeons' patient capacity.
Contact us today to explore how SubQ It! SU-25 fits into your surgical workflow, and learn more about this advanced system.
FAQs
1. What is a ligation clip?
A ligation clip is a small medical device used to clamp and close blood vessels or tubular structures during surgery. It provides faster and more reliable vessel occlusion than manual suture ligation, especially in laparoscopic procedures with limited access.
2. Are ligation clips considered implants?
Ligation clips are considered implantable devices, with most designed to remain in the body to maintain vessel occlusion. Non-absorbable clips remain permanently in situ, while absorbable clips degrade through hydrolysis, with resorption occurring over a variable period of weeks to months.
3. How effective is tubal ligation with clips?
Tubal ligation using clips is highly effective, with long-term failure rates typically below 1%. Outcomes depend on proper application technique and patient anatomy.
4. What materials are surgical ligation clips made from?
Ligation clips are made from three primary material types: medical-grade titanium for metal clips, inert polymers for non-absorbable clips, and bioabsorbable polymers for absorbable clips.
5. Can ligation clips cause complications?
While generally safe, complications can occur. These include clip migration, incomplete vessel occlusion causing bleeding, MRI artifacts with metal clips, and rare allergic reactions. Proper sizing and correct application minimize these risks.
6. Can ligation clips be used on all vessel sizes?
Ligation clips are typically used for small to medium vessels and ducts. They are not suitable for large vessels where higher pressure increases the risk of clip slippage or failure.