Skin closure decisions influence operative time, workflow, and post-operative care. Comparative data show mean closure times of 8.42 minutes for sutures versus 2.03 minutes for staplers, demonstrating how technique selection affects procedural efficiency.
While metal staples and sutures remain widely used, each involves trade-offs in speed and follow-up.
Bioabsorbable stapler applicators offer an alternative by placing absorbable fasteners beneath the skin, eliminating the need for removal while maintaining dermal support during healing.
In this blog, you’ll learn how to assess biodegradable staple applicators in 2026, including the clinical, operational, and material factors that determine the right choice for your practice.
Key Takeaways:
- Bioabsorbable stapler applicators place fasteners within the dermis, eliminating the need for removal after closure.
- Mechanical stapling methods are faster than suturing, improving efficiency in high-volume procedures.
- System performance depends on material behavior, applicator precision, and fastener design during early healing.
- Subcuticular placement avoids external skin staples, reducing visible puncture marks.
- Device selection should consider ease of use, compatibility with incision length, and overall workflow fit.
What Are Biodegradable Stapler Applicators?
Bioabsorbable stapler applicators are wound-closure devices that place absorbable fasteners within the dermal layer to approximate skin edges during incision closure.
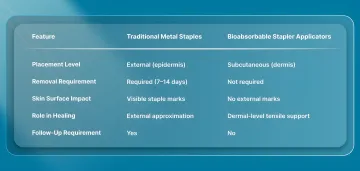
Unlike traditional metal skin staplers, which place external staples on the epidermis and require removal within 7 to 14 days, bioabsorbable systems deploy fasteners subcutaneously, beneath the skin. They remain there during healing and are gradually absorbed by the body.
In practice, this means:
- No external staple marks on the skin surface
- No follow-up visit for staple removal
- Closure occurs at the dermis level, where tensile support is most relevant during early healing.
A clear definition of biodegradable stapler applicators makes it easier to examine the essential components that form a complete bioabsorbable wound-closure system.
3 Core Components of Bioabsorbable Wound-Closure Systems
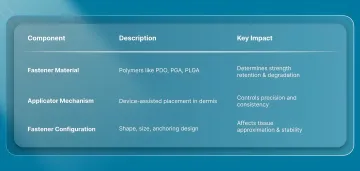
The clinical performance of a bioabsorbable wound-closure system depends on three key factors: the fastener material, the applicator mechanism, and the fastener design.
Each influences how the device performs during placement, how long it supports the wound, and how tissue responds during healing.
1. Bioabsorbable Fastener Material
Bioabsorbable closure systems are typically made from synthetic polymers such as polydioxanone (PDO), polyglycolic acid (PGA), or copolymers like poly(lactic-co-glycolic acid) (PLGA), all widely used in absorbable medical devices.
Material selection determines:
- How long does the fastener maintain tensile support
- The rate of degradation within the body
- The local tissue response during healing
These polymers are commonly used because they are biocompatible and designed to degrade predictably over time, allowing temporary mechanical support before being resorbed by the body.
Degradation occurs primarily through hydrolysis of ester bonds, producing byproducts such as lactic acid and glycolic acid, which are metabolized and cleared through normal physiological pathways.
2. Applicator Mechanism
The applicator determines how consistently and efficiently fasteners are placed within the dermal layer.
In bioabsorbable stapler systems, the device typically:
- Positions within the dermis just beneath the skin surface
- Uses a needle-based deployment mechanism to place the fastener
- Anchor the fastener across opposing wound edges before retracting
Some systems incorporate automatic needle retraction mechanisms to reduce needlestick risk, although this feature is device-specific rather than universal.
Systems such as SubQ It! SU-25 uses a handheld, device-assisted approach to deliver bioabsorbable fasteners beneath the skin in a controlled, repeatable manner. It is particularly relevant in longer incisions, where consistency and closure speed become more important.
3. Fastener Configuration
Fastener geometry, including shape, size, and anchoring design, determines how effectively the device approximates tissue.
Bioabsorbable fasteners are designed to:
- Engage the dermal layer on both sides of the incision
- Maintain tissue approximation during early healing
- Remain beneath the skin surface after deployment
Knowing how these systems are structured provides a practical foundation for evaluating which bioabsorbable stapler applicator to use.
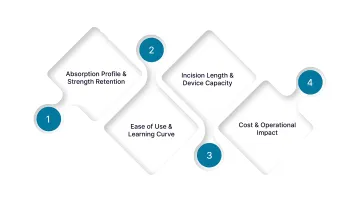
4 Factors to Consider When Choosing a Bioabsorbable Stapler Applicator
Evaluating a bioabsorbable stapler applicator requires more than comparing device features. The relevant question is how the system performs in the operating room, during healing, and across the full episode of care.
Below are the key factors to consider while choosing a bioabsorbable stapler applicator.
1. Absorption Profile and Strength Retention
The performance of a bioabsorbable fastener depends on how well it maintains tissue approximation during the early phases of healing.
Key considerations include:
- Whether the device provides adequate mechanical support during the initial healing period
- How gradually the material transfers the load from the device to the healing tissue
- Whether the degradation profile aligns with the tissue type and expected healing timeline
Surgeons should evaluate whether the system maintains sufficient stability during the period when wound separation risk is highest, particularly in higher-tension closures.
2. Ease of Use and Learning Curve
Adoption of any new closure system depends on how easily it integrates into existing surgical workflows.
Important factors include:
- Consistency of fastener deployment
- Clarity of device positioning within the dermal layer
- Availability of training and onboarding support
Subcuticular systems require accurate placement within the dermis, and outcomes depend on correct technique. Teams should ensure that adequate training resources are available before implementation.
3. Incision Length and Device Capacity
Device selection should align with the typical incision lengths encountered in your practice.
Different systems are designed to:
- Handle shorter incisions, including minimally invasive access points
- Accommodate longer incisions requiring multiple fasteners
The key consideration is whether the device allows efficient, continuous closure without requiring frequent repositioning or additional tools.
4. Cost and Operational Impact
The cost of a closure system should be evaluated in the context of the entire procedural workflow, not just the device price.
Relevant considerations include:
- Time required to complete skin closure
- Whether a follow-up visit for removal is required
- Impact on staff time and post-operative scheduling
Bioabsorbable systems eliminate the need for staple removal, thereby reducing postoperative workload and patient follow-up requirements.
Final Thoughts
Skin closure does not end with incision approximation. It continues to influence recovery management, follow-up structure, and the consistency of outcomes across different surgical settings.
As procedural demands increase, closure methods that reduce variability and compress operative time are becoming more relevant, particularly in longer incisions where manual suturing can extend case duration.
In this context, systems like SubQ It! SU-25 is designed for incisions up to 25 cm, using a device-assisted, subcuticular approach that can significantly reduce closure time while eliminating the need for staple removal.
To understand how SubQ It! SU-25 can improve efficiency in your current workflow, Contact us for more details.
FAQs
1. How long does it take for bioabsorbable staples to fully absorb?
Absorption varies with material and device design, typically taking weeks to several months. Clinical focus is on how long the device maintains adequate support during early healing rather than total absorption time.
2. Are bioabsorbable stapler applicators more expensive than traditional metal staplers?
Upfront costs are generally higher than those of traditional staplers or sutures. However, overall cost depends on factors such as operative time, follow-up requirements, and workflow efficiency.
3. What types of surgeries are best suited for bioabsorbable stapler applicators?
These systems are used across a range of procedures, including abdominal, gynecologic, orthopedic, and plastic surgeries. Suitability depends on incision type, length, and clinical requirements.
4. Do bioabsorbable staples provide the same tensile strength as metal staples?
Bioabsorbable fasteners are designed to provide sufficient strength during early healing. Performance depends on material properties, device design, and proper application.
5. What are the infection rates with bioabsorbable vs. traditional staples?
There is no consistent difference in infection rates across closure methods. Outcomes depend more on technique, tissue type, and patient factors than on the device alone.
6. How much training is required to use bioabsorbable staple applicators?
Training requirements vary by device. Most systems include guidance and support, with proficiency depending on familiarity with subcuticular placement techniques.