Closure decisions are often made quickly, yet they directly influence wound stability, follow-up requirements, and cosmetic outcomes. Even small variations in method or technique can result in avoidable complications.
As their use expands, cyanoacrylate-based closure methods are gaining wider adoption, with the global cyanoacrylate surgical sealants and adhesives market projected to reach USD 2.52 billion by 2035.
This growth reflects increasing clinical acceptance, although real-world performance still depends on appropriate case selection and precise application.
In this blog, you’ll explore how cyanoacrylate tissue adhesive should be used in 2026, including case selection, application technique, contraindications, and closure considerations.
Key Takeaways:
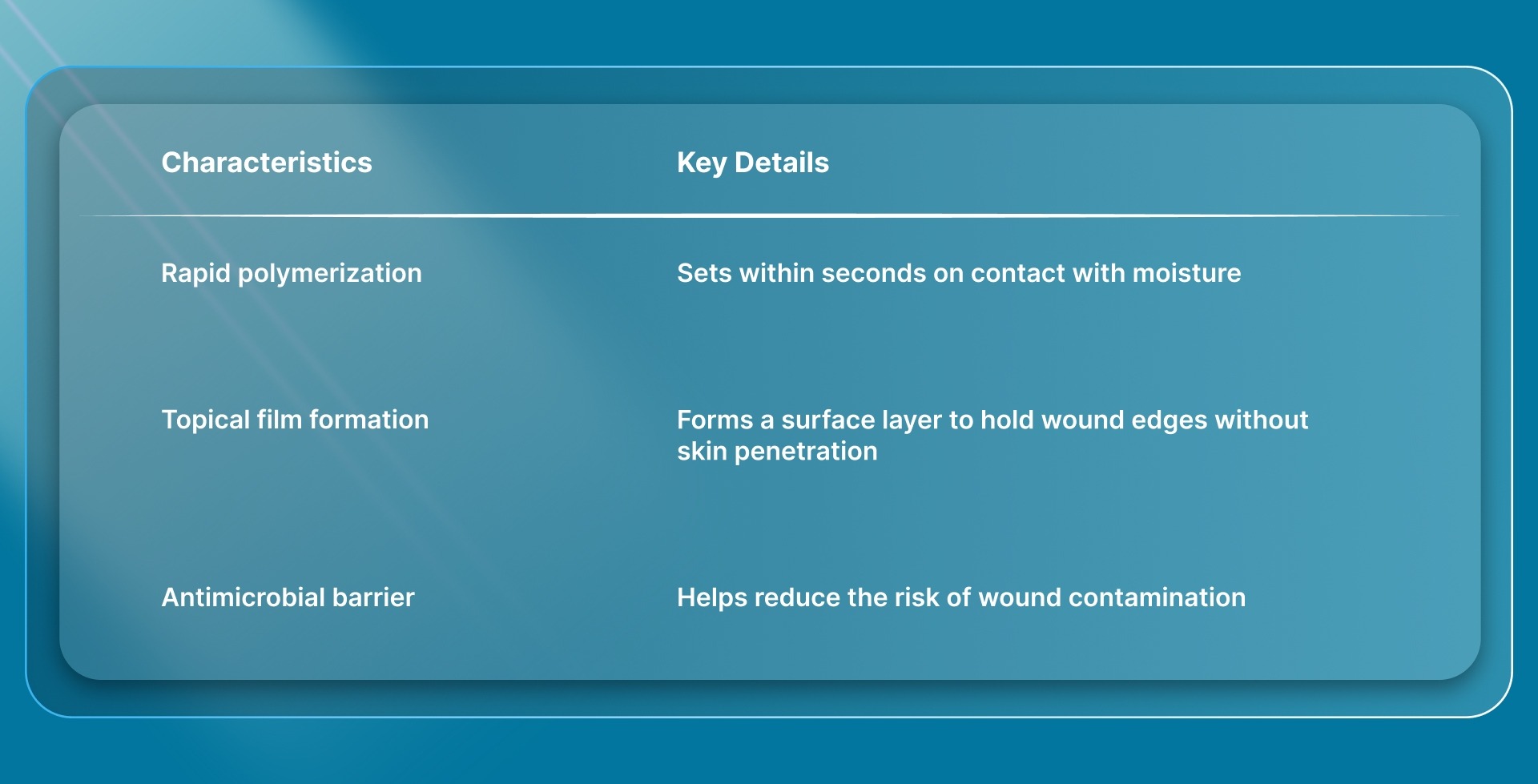
- Cyanoacrylate tissue adhesive is used for surface-level skin closure, where the adhesive bonds approximated wound edges quickly to form a protective layer.
- It works best on clean, low-tension wounds where edges can be easily aligned and maintained without additional support.
- Proper wound preparation, including cleaning, drying, and edge approximation, is essential to achieve consistent bonding and reliable closure.
- Cyanoacrylate tissue adhesive is not suitable for deep wounds, high-tension areas, contaminated wounds, or regions with significant movement.
- It reduces procedure time and eliminates the need for removal visits, but requires controlled application and a dry field for effective performance.
What is Cyanoacrylate Tissue Adhesive?
Cyanoacrylate tissue adhesive is a medical-grade liquid monomer used for superficial skin closure, bonding approximated wound edges when exposed to moisture.
In surgical practice, it functions as a topical (surface-level) closure method, forming a protective layer over the incision without penetrating the skin.
Cyanoacrylate tissue adhesive doesn’t require removal and sloughs off naturally in 5 to 10 days.
Here are the key characteristics of the cyanoacrylate tissue adhesive:
While cyanoacrylate tissue adhesive works at the surface level, subcutaneous systems such as SubQ It! SU-25 places bioabsorbable fasteners beneath the skin to provide internal approximation for longer or higher-tension incisions.
To understand how these adhesives differ in practice, it is important to look at the specific types available and how each is formulated for clinical use.
3 Types of Cyanoacrylate Tissue Adhesive
Different cyanoacrylate formulations vary in flexibility, strength, and handling characteristics, which influence their performance across surgical use cases.
For surgeons, selecting the appropriate type depends on wound tension, anatomical location, and expected movement at the closure site.
1. 2-Octyl Cyanoacrylate
2-octyl cyanoacrylate is one of the most commonly used formulations in surgical practice due to its balance of strength and flexibility. It is preferred in settings where the wound may be exposed to mild movement after closure.
- Higher Flexibility: Provides greater elasticity compared to shorter-chain cyanoacrylates, allowing the adhesive layer to tolerate limited movement without early failure
- Higher Tensile Strength: Offers stronger surface bonding than shorter-chain variants, making it more suitable for surgical incisions
- Clinical Use Cases: Commonly used for surgical incisions, pediatric closures, and areas with mild to moderate tension
2. n-Butyl Cyanoacrylate
n-butyl cyanoacrylate polymerizes quickly but forms a more rigid bond, making it suitable for controlled, low-movement environments. It is typically selected for smaller wounds where flexibility is less critical.
- Faster Polymerization: Sets rapidly on contact with moisture, supporting efficient application in straightforward cases.
- Lower Flexibility: Forms a more rigid film compared to 2-octyl formulations, limiting tolerance to movement
- Clinical Use Cases: Used for small, low-tension wounds where movement is minimal and controlled
3. Other Cyanoacrylate Variants
Other cyanoacrylate formulations exist but are not widely used in routine surgical workflows. These variants are primarily limited to investigational or specialized applications.
- Limited Clinical Adoption: Not commonly used in standard surgical practice due to limited widespread clinical use
- Variable Material Properties: Differences in molecular structure affect bonding strength, flexibility, and tissue response
- Use Cases: Primarily seen in research settings or niche clinical applications rather than routine wound closure
Recognizing the differences between these types clarifies the specific clinical situations in which cyanoacrylate tissue adhesive is most appropriate.
When Should You Use Cyanoacrylate Tissue Adhesive?
Cyanoacrylate tissue adhesive is used when the wound allows for reliable approximation of skin edges at the surface without requiring internal tensile support.
The decision is based on wound tension, edge quality, and the ability to maintain a dry field with minimal bleeding during application.
1. Ideal Wound Conditions
Cyanoacrylate tissue adhesive performs best when wound edges can be approximated easily and remain stable without additional support. These conditions directly affect bonding strength and overall closure reliability.
- Low-Tension Wounds: Edges come together without gaping or the need for deep sutures to maintain stability
- Clean, Linear Incisions: Smooth, well-defined edges allow uniform adhesive contact and consistent bonding
- Dry Field: Minimal bleeding or exudate is required to ensure proper polymerization and adhesion
2. Suitable Clinical Scenarios
This method is typically selected when wound characteristics support fast, surface-level closure without added complexity. It is most effective in controlled settings with predictable tissue behavior and minimal movement.
- Small Surgical Incisions: Common in minimally invasive procedures where rapid closure is beneficial
- Superficial Lacerations: Limited to the dermal layer without significant depth or structural complexity
- Pediatric Closures: Eliminates the need for removal, simplifying follow-up care and improving patient compliance
3. Intraoperative Considerations
Successful use depends on maintaining stable wound conditions during application and early bonding. Small variations in alignment, moisture, or access can affect the integrity of the closure.
- Stable Edge Approximation: Wound edges must remain aligned throughout application to ensure consistent bonding
- Controlled Application Environment: Clear visibility and access reduce the risk of adhesive misplacement or runoff
- Workflow Efficiency Goals: Selected when reducing closure time and avoiding follow-up removal visits is advantageous
Understanding when cyanoacrylate tissue adhesive is appropriate also makes it important to recognize the situations where it may not be the right choice.
When Cyanoacrylate Tissue Adhesive Should Not Be Used?
Cyanoacrylate tissue adhesive should be avoided when wound conditions do not support stable surface bonding or when additional structural support is required.
In these cases, adhesive-only closure can increase the risk of dehiscence or suboptimal healing.
- High-Tension Wounds: Edges cannot remain approximated without deep support, increasing the risk of bond failure and wound separation
- Contaminated or Infected Wounds: Surface sealing may trap bacteria and increase the risk of infection
- Irregular or Poorly Approximated Wounds: Uneven or jagged edges prevent consistent adhesive contact and reduce bond reliability
- Moist or Actively Bleeding Wounds: Excess blood or exudate interferes with polymerization, reducing bond strength
- Deep Wounds Without Subcutaneous Support: Lack of internal closure increases the risk of separation, as adhesive does not provide tensile strength
- High-Movement Areas: Regions over joints or mobile surfaces increase mechanical stress, which can disrupt the adhesive layer
Once you understand these limitations, it helps ensure the right preparation and clinical conditions are in place before application.
What You Need Before Using Cyanoacrylate Tissue Adhesive?
Effective use of cyanoacrylate tissue adhesive depends on proper wound preparation and controlled application conditions. Preparation directly affects polymerization, bonding strength, and overall closure reliability.
Here’s what you need before using cyanoacrylate tissue adhesive:
- Wound Cleansing and Irrigation: Clean the wound thoroughly using sterile saline or a standard antiseptic solution to remove debris and contaminants before application
- Complete Hemostasis: Achieve full bleeding control using pressure or topical vasoconstrictors, as active bleeding can interfere with adhesive bonding
- Dry Wound Surface: Ensure wound edges are free of excess moisture or exudate to support proper polymerization and adhesion
- Edge Approximation Tools: Use fingers, forceps, or skin approximation devices to maintain precise and stable alignment during application
- Topical Anesthesia (If Needed): Apply before preparation in sensitive cases, as the adhesive application itself does not require injected anesthesia
- Controlled Application Environment: Maintain clear visibility, adequate lighting, and access to prevent adhesive runoff into adjacent areas
Once the necessary preparation is complete, the application process can be carried out in a structured and controlled manner.
9 Steps to Take to Use Cyanoacrylate Tissue Adhesive
Successful application depends on following a controlled, step-by-step sequence to ensure proper polymerization and stable wound closure. Each step must be performed correctly to avoid bonding failure or disruption of wound alignment.
1. Position the Wound Before Application
Position the wound to maintain control over adhesive flow during application. This helps prevent unintended spread into surrounding areas.
- Align the wound to minimize adhesive runoff due to gravity
- Protect adjacent areas such as eyes, hair, or mucosal surfaces
2. Achieve Complete Hemostasis and Dry the Wound
Ensure bleeding is fully controlled before applying the adhesive. A dry surface is required for effective polymerization and bonding.
- Use pressure or appropriate topical measures to stop bleeding
- Gently dry the wound edges to remove excess moisture or exudate
3. Approximate the Wound Edges Precisely
Bring the wound edges together to align evenly, with no gaps or overlap. Proper approximation is essential for consistent bonding.
- Use fingers, forceps, or an approximation device for alignment
- Maintain stable positioning during application
4. Activate the Adhesive Applicator
Prepare the adhesive device according to its design to ensure controlled delivery. Incorrect activation can result in excess adhesive or poor application control.
- Activate the applicator (e.g., crush or press the internal ampule)
- Bring adhesive to the tip without applying excessive pressure
5. Apply Adhesive Over the Wound Surface
Apply the adhesive along the approximated edges of the surface, not inside the wound. This ensures effective bonding without interfering with healing.
- Use gentle brushing motions along the wound line
- Keep the adhesive confined to the external surface
6. Extend the Adhesive Beyond the Wound Margins
Extend the adhesive slightly beyond the wound edges to improve bonding stability. This increases the surface area supporting closure.
- Apply adhesive slightly beyond each wound edge
- Ensure even coverage along the wound length
7. Hold the Wound in Position During Initial Setting
Maintain wound edge alignment while the adhesive begins to set. Movement during this phase can weaken the bond.
- Hold edges together until initial polymerization begins (typically around 30 seconds)
- Avoid releasing pressure too early
8. Apply Additional Thin Layers
Apply multiple thin layers to improve overall bond strength and durability. Thick applications can interfere with proper polymerization.
- Apply 2–3 thin layers rather than a single thick layer
- Allow each layer to dry before applying the next
9. Allow the Adhesive to Fully Cure
Allow the adhesive to fully set before completing the procedure. Disturbing the area too early can compromise the integrity of the closure.
- Allow the adhesive to cure for several minutes without disturbance
- Avoid touching or applying pressure during final setting
Understanding how the adhesive is applied provides useful context for evaluating its practical advantages and clinical limitations.
Benefits and Limitations of Cyanoacrylate Tissue Adhesives
Cyanoacrylate tissue adhesives provide a fast, surface-level closure option in appropriately selected cases. Their effectiveness depends on wound characteristics, particularly tension, moisture, and edge quality.
Below are the benefits and limitations of cyanoacrylate tissue adhesives.
A clear view of the benefits and limitations helps shape how the adhesive should be applied in day-to-day clinical practice.
Best Practices for Using Cyanoacrylate Tissue Adhesive Effectively
Effective use of cyanoacrylate tissue adhesive depends on consistent technique and controlled application. These practices help maintain bond integrity and reduce the risk of bond failure or early dehiscence.
- Maintain Precise Edge Alignment: Keep wound edges evenly approximated throughout application, as minor shifts can weaken bond integrity.
- Use Thin, Controlled Layers: Apply multiple thin layers rather than a thick coating to support proper polymerization and consistent bonding.
- Avoid Adhesive Entry Into the Wound: Apply only on the surface to prevent interference with healing and maintain proper closure.
- Control Adhesive Flow: Use minimal pressure during application to avoid excess adhesive or unintended spread.
- Allow Adequate Time Between Layers: Let each layer set before applying the next to build a stable adhesive film
- Minimize Movement During Initial Setting: Keep the wound stable during early polymerization to prevent disruption of the bond
- Avoid Contact With Absorbent Materials: Prevent contact with gauze or fabric, as this can trigger heat generation and affect bond integrity
Final Thoughts
Cyanoacrylate tissue adhesive supports surface closure, but variations in tension, depth, and tissue behavior determine when surface bonding alone is sufficient.
As expectations for reliability and efficiency increase, the need for closure methods that perform consistently beyond low-tension scenarios becomes more relevant in routine practice.
In this context, systems like SubQ It! SU-25 provides a subcutaneous, device-assisted approach that places 25 bioabsorbable fasteners to close incisions up to 25 cm.
This allows coverage of cases that would otherwise require lengthy manual suturing, while also saving approximately 25 minutes of OR time per procedure.
Contact us today to explore how SubQ It! SU-25 fits into your closure workflow and learn about its role in your practice.
FAQs
1. Can cyanoacrylate tissue adhesive be used in patients with sensitive skin?
Yes, it can be used in most cases, but some patients may develop mild contact dermatitis. Prior sensitivity to adhesives or repeated exposure may increase this risk.
2. Does cyanoacrylate tissue adhesive provide antimicrobial protection?
Cyanoacrylate adhesives form a protective barrier that can limit bacterial penetration. However, they should not replace proper wound-cleansing or infection-control practices.
3. Can the adhesive be reapplied if the bond fails early?
Reapplication may be considered if the wound remains clean and well-approximated. The wound should be reassessed to determine whether adhesive closure remains appropriate.
4. Are there any storage or handling considerations for cyanoacrylate adhesives?
Yes, they should be stored according to manufacturer guidelines to prevent premature polymerization. Exposure to moisture or heat can affect shelf life and performance.
5. Can cyanoacrylate tissue adhesive be used in combination with dressings?
Yes, while the adhesive forms a protective surface barrier, additional dressings may be used in areas exposed to friction or contamination.
6. Can cyanoacrylate tissue adhesive be used in patients with comorbidities such as diabetes?
It can be used in selected cases, but wound healing may be slower in patients with conditions such as diabetes. Careful patient selection and monitoring are important for optimal outcomes.