The scissors that worked well earlier may not be the ideal match for the procedures you're running today. As your case mix evolves, so should the instruments on your tray.
The number of scissor designs available today is somewhere around 2,000, spanning every blade material, tip profile, and length on the market. Matching the right scissor to the right tissue is a practical efficiency decision. Scissors that don't match the tissue type force extra passes and add extra minutes to the entire procedure.
This post covers the best surgical scissors by specialty and tissue type, compares blade materials and sizing, and shows how your scissor selection connects to the closure step of the workflow.
Key Takeaways
- Surgical scissors serve both cutting and blunt dissection functions, and matching the right type to the tissue directly affects operative precision and speed.
- Metzenbaum scissors are built for delicate tissue dissection, while Mayo scissors handle fascia, heavy tissue, and suture cutting.
- Iris scissors are the preferred choice for fine work on the head, neck, and small-incision cases in plastic surgery.
- A scissor's cutting edge can be angled anywhere from 0 to 15 degrees, with steeper angles suited to soft tissue and shallower angles to denser structures.
- Reusable cutting instruments start losing performance after just 5 autoclave cycles, making maintenance and replacement timing a real performance factor.
What Are Surgical Scissors and How Are They Classified?
Surgical scissors are handheld cutting instruments used for tissue dissection, blunt separation of tissue planes, and suture cutting. How well a surgeon knows the biomechanics of each scissor type has a direct effect on operative outcomes, according to a 2024 review in the Journal of Surgical Orthopedic Advances.
The three core variables that define any surgical scissor are design (blade shape and shank-to-blade ratio), blade material (stainless steel, tungsten carbide, or SuperCut), and size (length, tip configuration, and curvature). Each variable should match the tissue being handled and the procedure being performed.
Surgeons today can choose from a variety of designs, ranging from standard operating surgery scissors to highly specialized microsurgical instruments. Picking the right pair starts with understanding what each type is built to do.
Which Surgical Scissors Work Best for Each Specialty?
The best surgical scissors for any given case depend on the tissue type, the depth of the operative field, and the precision required. Here's how the major scissor types compare across specialties.
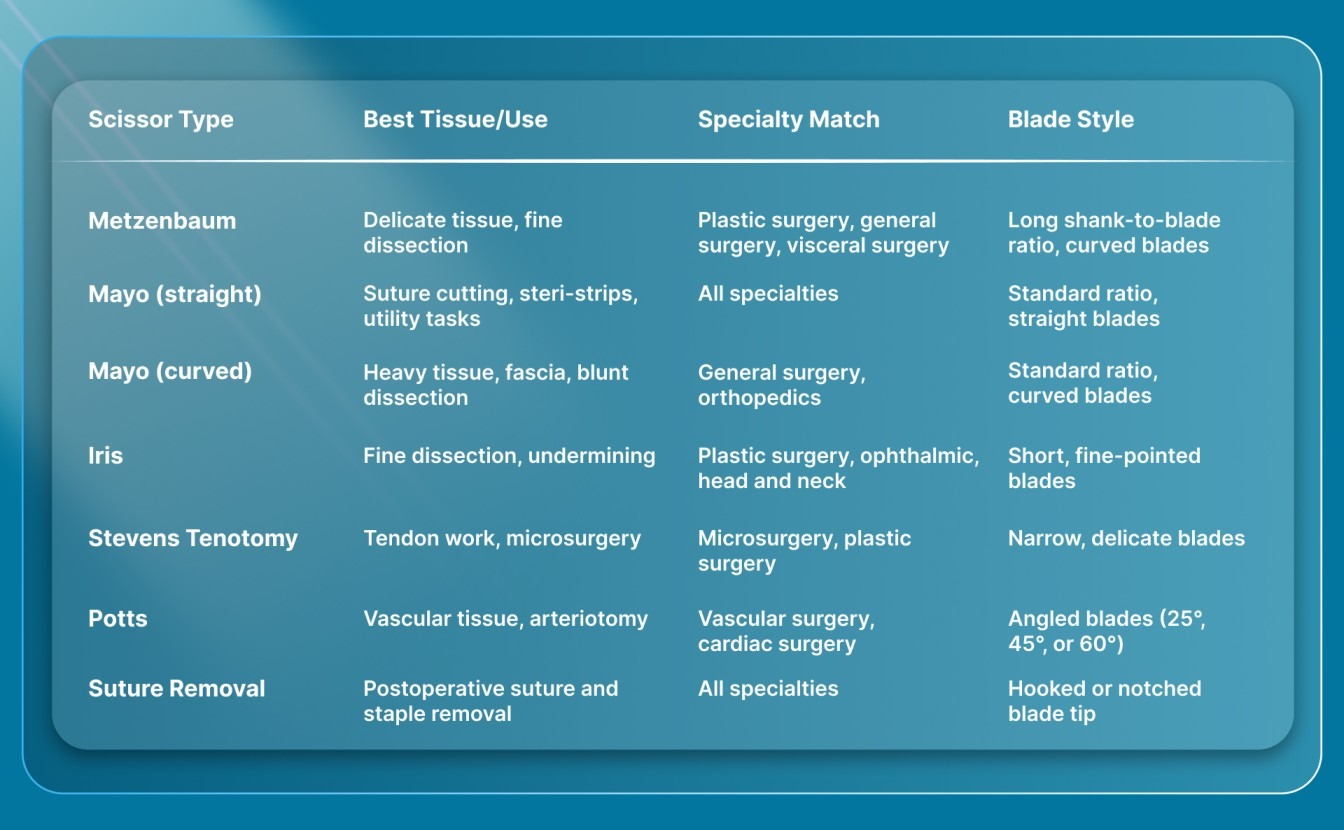
Each type earns its place on the tray for a specific reason. Here's a closer look at the ones that come up in nearly every operative set.
Metzenbaum Scissors
What sets Metzenbaum scissors apart is a longer shank relative to the blade, combined with a narrower tip profile than you'd find on a Mayo. That geometry makes them the go-to for delicate tissue dissection and fine plane development, giving reach into deeper fields without sacrificing control.
In visceral surgery specifically, the standard curved Metzenbaum remains the default dissecting scissor. Robust variants with heavier blades exist for gynecologic and orthopedic procedures where tissue resistance is higher.
Mayo Scissors
When you need to trim a suture, peel a steri-strip, or cut an electrode lead, a straight Mayo is the standard reach. It's the workhorse cutter on most trays, built for non-tissue tasks where precision matters less than a clean, reliable cut.
Curved Mayo scissors serve a different role entirely. Their sturdier construction handles fascia, heavy connective tissue, and blunt dissection in deeper operative fields. They're standard in general and orthopedic surgical shears sets.
Iris Scissors
For fine-field work on the head and neck, Iris scissors are the instrument surgeons reach for most often. Their short, fine-pointed blades give the control needed for undermining skin flaps, excising small lesions, and working in tight operative windows during plastic, ophthalmic, and dermatologic cases.
For surgeons who handle laparoscopic port-site closures or small incisions routinely, Iris scissors also serve well for trimming tissue at trocar sites before closure.
Stevens Tenotomy Scissors
Stevens tenotomy scissors offer an even narrower blade profile than Iris scissors, with a delicate build designed for tendon work and microsurgical dissection. They're a staple in microsurgery and plastic surgery trays where the operative field is small, and the tissue tolerance for error is minimal.
Their fine tips make them useful for separating tissue layers in confined spaces, particularly around tendons, nerves, and small vessels. If your case mix includes hand surgery, facial reconstruction, or any procedure requiring sub-millimeter control, Stevens tenotomy scissors belong on the tray.
Potts Scissors
Potts scissors are built specifically for vascular work. Their angled blade tips (available in 25°, 45°, and 60° configurations) let surgeons make precise arteriotomy cuts without compressing or distorting the vessel wall.
The angled design is what makes these distinct from any other scissor type. A straight-bladed scissor forces an awkward approach angle on a vessel, increasing the risk of an uneven cut. Potts scissors remove that problem, which is why they're standard on vascular and cardiac surgery trays.
Suture Removal Scissors
Suture removal scissors, like the Spencer and Littauer, have a hooked or notched blade tip that lifts the suture away from the skin before cutting. These are postoperative instruments, not intraoperative dissecting tools, and they belong in every clinic's scissors and stitches removal kit.
The hook design matters because it prevents the blade from pressing directly into the skin surface during removal. For practices that still use traditional sutures or metal staples requiring a return visit, having a dedicated removal scissor speeds up the process and reduces patient discomfort.
How Does Blade Material Affect Scissor Performance?
Blade material determines how long a scissor holds its edge, how cleanly it cuts, and how much it costs to replace. The three materials you'll see across surgical scissors today are standard stainless steel, tungsten carbide inserts, and SuperCut blades.
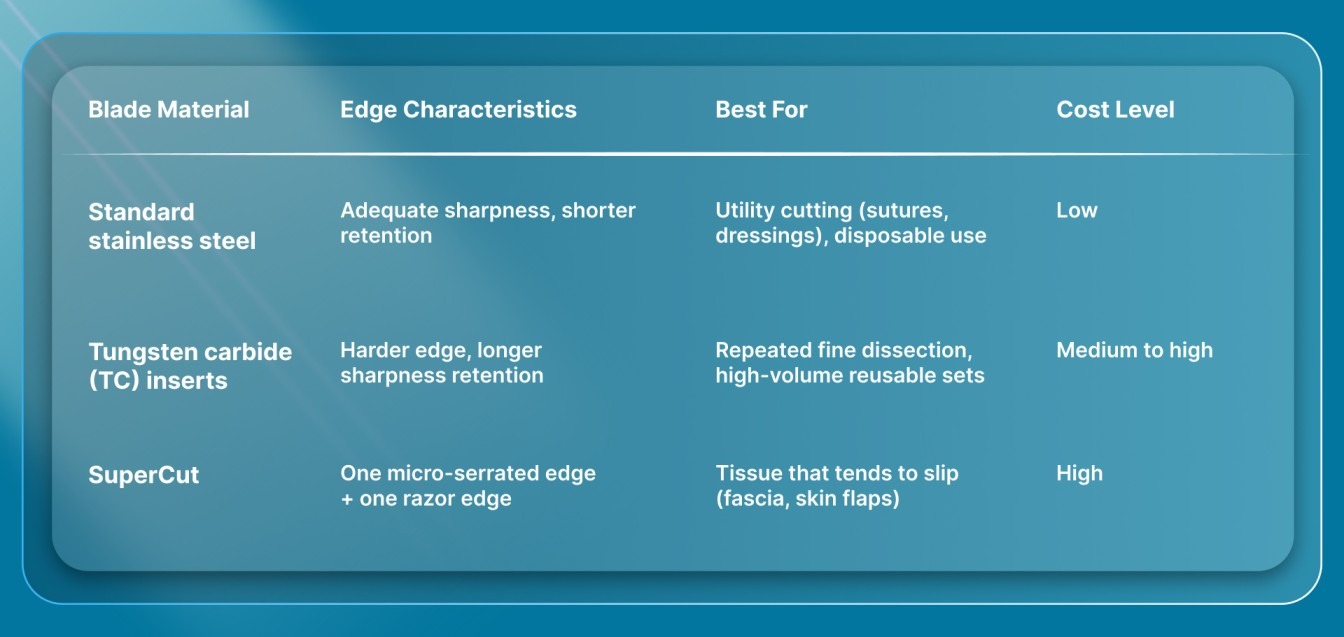
Tungsten carbide inserts are widely reported to retain sharpness longer than standard stainless steel, though no peer-reviewed controlled trial has published a specific multiplier comparing the two materials head-to-head. The practical consensus among surgeons is that TC scissors maintain their cutting edge across more cases before requiring resharpening.
SuperCut technology pairs one micro-serrated blade with one razor-sharp blade. The serrated side grips tissue to prevent slippage while the smooth side delivers a clean cut. This is particularly useful when working with fascia or slippery tissue planes, though the added manufacturing cost puts SuperCut skin scissors at a higher price point than standard or TC options.
For surgeons in private practice who control their own instrument budgets, the choice often comes down to case volume. High-volume dissection work justifies the TC or SuperCut investment. Lower-volume utility cutting (suture trimming, dressing removal) doesn't require the premium blade.
What Size and Tip Configuration Should You Choose?
Surgical scissors range from roughly 9 cm (Iris) to 23 cm (long Metzenbaum and Mayo), and the right length depends on the depth of the operative field and the tissue being handled.
- Short scissors (9-12 cm): Iris and Stevens tenotomy. Built for superficial, fine-detail work. Head and neck, dermatologic, and ophthalmic procedures.
- Medium scissors (14-18 cm): Standard Metzenbaum and Mayo. General-purpose dissection and cutting in abdominal, breast, and extremity cases.
- Long scissors (20-23 cm): Extended Metzenbaum and deep-cavity Mayo. Necessary for pelvic, thoracic, and deep abdominal dissection where reach is critical.
Tip configuration adds another decision layer. Curved tips follow tissue planes more naturally during blunt dissection, which is why curved Metzenbaum and curved Mayo are far more common in operative sets than their straight counterparts. Straight tips are reserved for suture cutting and tasks where a linear cut path matters.
Tip sharpness profiles (blunt/blunt, sharp/blunt, sharp/sharp) serve specific safety functions. Sharp/blunt combinations protect underlying structures during dissection near critical anatomy. Blunt/blunt tips are safest for blunt spreading in deep cavities. Sharp/sharp tips provide the cleanest cuts but carry the highest risk of inadvertent tissue injury and are typically limited to scalpel blades and surface-level cutting tasks.
How Does Blade Sharpness Change With Sterilization and Use?
Blade sharpness isn't static. Every reusable surgical scissor degrades with repeated use and sterilization, and the rate of that degradation affects both cutting performance and safety.
How sharp a surgical scissor feels in your hand depends on its blade-edge geometry. The angle of the cutting surface can range from 0 degrees to 15 degrees. A steeper angle (closer to 15 degrees) produces an extremely sharp edge suited for soft tissues like conjunctiva, while a shallower angle holds up better against denser structures. When that edge geometry dulls, the scissor requires more force to cut, which increases tissue trauma and slows the case.
Every autoclave cycle pushes heat through your instruments at 121°C to 134°C for 15 to 30 minutes. Factor in the full turnaround, including cool-down, and each reprocessing run takes roughly 1 hour, with an ideal 5-hour rest period before the instruments go back into service.
After about 5 autoclave cycles, you can start to measure a real drop in how well reusable cutting instruments perform, according to a systematic review and network meta-analysis. By 15 cycles, the decline is steep. That study tested endodontic instruments specifically, though the underlying mechanism (repeated heat exposure wearing down the cutting edge) applies to any reusable blade. A separate 2022 pilot study added another layer: instruments that had lost sharpness also retained more biological material after standard sterilization, while PVD-coated instruments stayed significantly cleaner.
For practical purposes, this means tracking your scissors through suture removal scissors and dissecting sets alike. Scheduling resharpening or replacement before the 5-cycle threshold maintains consistent cutting performance and reduces the risk of excessive force during dissection.
How Does Scissor Choice Connect to Wound Closure?
Dissection and cutting are only part of the operative workflow. The instruments you choose for closure affect OR time, scarring outcomes, and whether the patient needs a return visit for staple or suture removal.
Traditional metal staples close quickly but are placed on the skin surface and must be removed in 7 to 10 days. That removal visit adds to the practice's scheduling burden and leaves characteristic railroad-track scars where the staple legs pierced the skin. Hand-sewn subcuticular suture avoids surface puncture marks, but it costs time. In a 4,311-patient mastectomy series, surgeons who closed with absorbable subcuticular stapling finished in 16.2 minutes on average, while hand-sewn cases took 36.5 minutes, with no difference in infection rates.
SubQ It! is a bioabsorbable subcutaneous wound closure system that places dissolving dermal fasteners under the skin. The fasteners dissolve naturally, so there's no removal visit and no railroad-track scarring. SubQ It! SU-10 holds 10 fasteners for incisions up to 10 cm, including very small laparoscopic trocar sites where surface-applied devices can't operate. SubQ It! SU-25 holds 25 fasteners for incisions up to 25 cm, covering longer closures in open and plastic surgery cases.
Pairing precise dissecting scissors with an efficient absorbable closure device means the time you save with good instrument selection doesn't get lost at the closure step. The workflow holds together from first cut to final fastener.
What Should Surgeons Consider When Buying Surgical Scissors?
The right purchasing approach depends on your case mix, practice model, and instrument maintenance. Here are the factors that matter most.
- Case mix alignment: Stock scissors that match the tissues and procedures you perform weekly. A plastic surgery practice needs Metzenbaum and Iris in regular rotation. A general surgery practice needs curved Mayo for fascia and Metzenbaum for finer planes.
- Blade material vs. volume: Tungsten carbide and SuperCut justify their cost when you're doing high-volume dissection work. For utility tasks like suture cutting, standard stainless is sufficient.
- Reusable vs. disposable trade-off: Every cost analysis in a 2024 systematic review of laparoscopic instruments (11 studies total) pointed in the same direction: disposable devices cost significantly more than their reusable counterparts. Reusable scissors cost more upfront but amortize over dozens or hundreds of cases, as long as you track sterilization cycles and resharpening schedules.
- Tip configuration: Match curved vs. straight and sharp/blunt profiles to your most common dissection needs. Curved tips are the default for tissue dissection. Straight tips are best suited for utility and suture-cutting roles.
- Closure instruments too: The same purchasing rigor you apply to your dissecting scissors should extend to your closure devices. A well-stocked tray includes the right best skin stapler or closure system for each incision type.
Instrument purchasing works best when you evaluate the full tray together, from dissection through closure, rather than replacing one scissor at a time.
Final Thoughts
The best surgical scissors match the tissue, the procedure, and the surgeon's case mix. Metzenbaum handles delicate dissection. Mayo handles heavy tissue and utility cutting. Iris handles fine-detail work in small fields. Blade material and maintenance timing determine how long each scissor performs at its best.
Building an instrument tray that performs consistently means evaluating every step of the operative workflow together. The scissors you use for dissection set the pace, and the closure system you choose determines whether that efficiency carries through to the end of the case.
SubQ It! is a bioabsorbable wound closure system that places dissolving fasteners under the skin, with options from small laparoscopic incisions up to 25 cm. Fasteners dissolve naturally with no removal visit and no railroad-track scarring. When your dissecting instruments are dialed in, and your closure system keeps pace, the whole workflow gets faster. Contact us today to see how SubQ It! fits your instrument tray.
FAQs
1. How Often Should Surgical Scissors Be Resharpened?
Resharpening frequency depends on case volume and tissue type, but cutting performance tends to decline noticeably after several sterilization cycles. A good rule is to inspect blade alignment and test cutting quality at regular intervals rather than waiting for obvious dullness.
2. Can You Autoclave Tungsten Carbide Scissors?
Yes, tungsten carbide scissors are designed to withstand standard steam autoclaving at the same temperatures used for stainless steel instruments. The carbide inserts are bonded to the blade tips and tolerate repeated heat sterilization without loosening under normal conditions.
3. Are Disposable Surgical Scissors Reliable for Complex Cases?
Yes, disposable scissors deliver consistent sharpness because they're used once and discarded, avoiding the degradation that affects reusable instruments over time. They're most common in laparoscopic and single-use instrument sets.
4. What Is the Difference Between Curved and Straight Surgical Scissors?
Curved scissors follow tissue planes during blunt dissection, making them the default for most operative dissection tasks. Straight scissors provide a linear cutting path and are typically reserved for suture cutting, steri-strip trimming, and other utility tasks.
5. Do SuperCut Scissors Work on All Tissue Types?
No, SuperCut scissors are designed primarily for tissues that tend to slip during cutting, like fascia and skin flaps. For standard suture cutting or heavy bone-adjacent dissection, a traditional blade configuration is typically more practical.
6. How Long Do Tungsten Carbide Scissors Last Before Replacement?
Lifespan varies with case volume and sterilization frequency. Tungsten carbide retains its edge longer than standard stainless steel, and many surgeons report getting several months to over a year of regular use before replacement is needed.