Most surgeons know manual subcuticular suturing takes real OR time. Most also know metal staples leave marks that patients notice. The compromise you made years ago between speed and cosmetic quality is one worth revisiting.
Data now shows sutureless methods cover a wider range of incisions than they did a decade ago. In fact, sutureless methods offer closure times that are nearly half those of hand-sewn sutures.
This post covers every practical sutureless option in detail, where each one fits, and how to choose the right method for skin closure.
Key Takeaways
- Sutureless skin closure covers tissue adhesives, adhesive strips, zipper devices, and bioabsorbable subcuticular staplers, each with a specific case-type fit.
- Zipper-style devices save about 4.9 minutes per closure versus suture but score lower on one-month scar scales.
- Absorbable subcuticular staplers cut closure time from 36.5 minutes to 16.2 minutes in one mastectomy series, with matched infection rates.
- Published OR-minute cost averages around $46.04 per minute, so closure time translates directly into recoverable capacity.
- No single sutureless method fits every case. Contamination, tension, hair density, and anatomy all narrow the options.
What Is Sutureless Skin Closure?
Sutureless skin closure is any method that approximates skin edges without a traditional needle-threaded suture on the surface. That includes tissue adhesives, adhesive strips, external zipper devices, and bioabsorbable subcuticular staplers placed under the skin.
Across these methods, the closure material either sheds on its own or stays inside the body to dissolve. Most cyanoacrylate adhesives, for example, polymerize within around 2.5 minutes and shed in 5 to 10 days as the skin underneath re-epithelializes. No removal visit is required.
A common example is laparoscopic trocar closure. A surgeon can close each port site with a sutureless method and send the patient home without scheduling a staple-removal follow-up. That single change removes friction from the OR and the post-op clinic schedule. For surgeons reviewing their defaults, the broader category breakdown on types of skin closure and alternative suture closure methods is worth a look.
Why Are Surgeons Moving Away from Traditional Sutures and Staples?
Surgeons are moving away from traditional sutures and staples because the OR cost of manual suturing and the wound morbidity and cosmetic cost of metal staples have become harder to justify. Published trial data now give closure choices a quantitative floor to work from, and patient-reported scar scores consistently favor subcuticular methods over staples.
Here's what's driving the shift:
- OR time pressure: Each operating room minute runs around $46.04 on average across U.S. studies, making every closure minute a real budget line item.
- Wound complications: A pooled analysis of cesarean closures found metal staples carried a relative risk of 1.88 for wound complications compared with subcuticular suture.
- Patient-reported scar quality: In a randomized cesarean study, patients closed with subcuticular suture rated scar appearance higher than patients closed with staples on POSAS scales.
- Return-visit obligation: Metal staples need to come out in 7 to 10 days, which creates a follow-up burden on both the patient and the clinic.
- Infection burden: Surgical site infections affect 0.5% to 3% of U.S. surgical patients, and superficial incisional infections make up more than 50% of all SSIs, making closure choice one of the controllable variables.
The sutures vs. staples decision rarely comes down to one variable. It's a combination of closure time, complication risk, and how the patient experiences the scar months later.
What Are the Main Types of Sutureless Skin Closure Methods?
The main types of sutureless skin closure are tissue adhesives, adhesive skin closure strips, external zipper-style devices, and bioabsorbable subcuticular staplers. Each works on a different mechanism and fits a different case profile, so surgeons typically keep more than one option in their closure toolkit.
Here's a quick side-by-side overview of how these methods compare on the variables that matter most in the OR:
| Method | Best Use Case | Closure Speed | Scar Profile | Removal Needed | Incision Length Coverage |
|---|---|---|---|---|---|
| Tissue adhesives | Low-tension facial and small lacerations | Fast (polymerizes in ~2.5 min) | Matches suture by month 3 | No (sheds in 5–10 days) | Small to moderate |
| Adhesive closure strips | Shallow, low-tension wounds | Fast | Variable, tension-dependent | Falls off or peels | Small |
| Zipper-style devices | Low-to-moderate tension linear wounds | ~4.9 min faster than suture | Lower 1-month scar scores than suture | Peeled off | Small to moderate |
| Bioabsorbable subcuticular staplers | Small laparoscopic to longer open incisions | Faster than hand-sewn suture | Subcuticular-grade cosmesis | No (dissolves under skin) | Very small to 25 cm |
Here’s a detailed breakdown of each method:
Tissue Adhesives (Cyanoacrylate Glues)
Cyanoacrylate tissue adhesives bond epithelial edges through a fast polymerization reaction. A 2023 meta-analysis of 18 randomized trials covering 1,020 patients with facial or neck wounds found adhesives produced better physician-rated cosmetic scores than sutures at one month, with equivalence by three months.
The practical win is that adhesives skip the return visit. The trade-off is tension tolerance. They don't hold on joints, high-mobility areas, or anywhere deeper support hasn't already been placed.
Adhesive Skin Closure Strips
Adhesive strips attach to the surface and pull wound edges together through tension distribution across the skin. They're quick to apply and have no associated removal procedure, since they peel off or fall away on their own.
The limitation is similar to tissue adhesives. Strips need clean, dry, low-tension skin to hold. On hair-bearing areas or moist sites, adhesion drops quickly. For surgeons working with reinforced closure strips on linear wounds, the fit is narrow but useful.
Zipper-Style External Devices
Zipper-style devices use an adhesive base with a central tensioning mechanism that pulls edges together. A 2024 systematic review of ten studies found these devices cut closure time by around 4.9 minutes per wound versus suture, with infection and dehiscence rates broadly similar.
The scar data was less favorable. At the one-month mark, scar scale scores came in below suture closures in the same review. Zipper devices remain on the skin surface, which limits their fit for cosmetically sensitive sites and high-tension wounds.
Subcuticular Absorbable Sutures
Subcuticular absorbable sutures aren't technically sutureless, but they belong in the comparison because they share the no-removal benefit. The closure material stays under the skin and dissolves over weeks. The trade-off is time. Hand-sewn subcuticular closure remains slow, especially on longer incisions.
Bioabsorbable Subcuticular Staplers
For surgeons who want stapler speed without the cosmetic penalty of metal staples or the time cost of hand-sewn suture, bioabsorbable subcuticular staplers are the option most often overlooked. These devices deliver dissolving fasteners under the skin, pairing rapid deployment with subcuticular-grade cosmetic outcomes.
A single-center retrospective study of 4,311 mastectomy patients showed absorbable subcuticular stapling averaged 16.2 minutes per closure versus 36.5 minutes for hand-sewn subcuticular suture, with matched SSI rates between the two groups.
SubQ It! builds directly on this approach. The SubQ It! SU-10 closes incisions up to 10 cm and fits very small laparoscopic port sites where surface-applied devices cannot operate. The SubQ It! SU-25 handles incisions up to 25 cm, which covers open general and plastic cases.
The dermal fasteners are bioabsorbable and placed under the skin, which means no removal visit and no external puncture marks along the incision line.
How Do You Choose the Right Sutureless Skin Closure for Each Case?
Choosing the right sutureless skin closure method comes down to four variables that filter your options quickly. Incision length, wound tension, anatomical site, and contamination status narrow the field before cosmetic priority or speed preference factors in.
Here's a practical decision flow:
- Assess contamination status first: Dirty, infected, or bite wounds rule out tissue adhesives, strips, and zipper devices across the board. These cases generally need traditional skin closure sutures or alternative approaches.
- Check wound tension: High-tension areas like joints, back, and scalp need either deep subcuticular support or a stapler-based method. Surface adhesives and strips fail here.
- Measure incision length: Short facial lacerations suit tissue adhesives. Moderate linear incisions can take zipper devices or adhesives. Longer incisions up to 25 cm are where bioabsorbable subcuticular staplers show their strongest time advantage.
- Evaluate anatomical site: Hair-bearing areas reduce adhesive and strip adhesion. Mucosal surfaces rule out adhesives entirely. Subcuticular methods, including staplers, sidestep most of these site restrictions.
- Factor in cosmetic priority: Cosmetically sensitive sites favor subcuticular methods or tissue adhesives, both of which avoid surface puncture marks.
Once these filters run, you're usually left with one or two viable methods per case. Matching method to case this way reduces dehiscence risk, minimizes cosmetic complaints, and keeps OR time predictable across your schedule.
What Are the Cosmetic and Clinical Outcomes Across Methods?
Cosmetic and clinical outcomes vary meaningfully across sutureless methods, and the differences are documented in randomized and prospective studies. Metal staples carry a consistent scar-score penalty compared with subcuticular closure, while adhesives and staplers tend to match suture-grade outcomes on both cosmesis and infection.
Here's what the evidence shows:
- Adhesive cosmesis: Physician-rated cosmetic scores favored cyanoacrylate over sutures at one month on facial wounds, with parity by month three.
- Staple vs. suture scarring: Patients closed with subcuticular suture reported better scar appearance than patients closed with metal staples, and independent observer scores favored the suture group on the same wounds.
- Absorbable stapler infection rates: In the mastectomy series referenced earlier, SSI rates were statistically indistinguishable between absorbable subcuticular staplers and hand-sewn suture.
- Zipper device scar scores: At one month post-closure, zipper devices scored lower than sutures on scar scales in the 2024 meta-analysis.
- Adhesive contact dermatitis: Reported rates of allergic contact dermatitis to 2-octyl cyanoacrylate adhesives have ranged from 0.5% to 14% across published studies.
The outcome data points toward subcuticular methods and tissue adhesives for cosmetically sensitive work, with staplers gaining ground on longer incisions where time-per-closure matters most.
What Does Sutureless Skin Closure Mean for OR Efficiency and Practice ROI?
Sutureless skin closure has a measurable effect on OR efficiency because every minute shaved off closure translates directly into recoverable OR capacity at a known per-minute cost. U.S. data puts the mean cost of OR time at around $46.04 per minute, which lets surgeons and practice managers quantify closure choice in real dollars.
The method with the largest documented time delta is absorbable subcuticular stapling. In the mastectomy series covered earlier, closure averaged 20.3 minutes shorter with an absorbable stapler than with a hand-sewn subcuticular suture, per case. That's meaningful recoverable capacity across a high-volume schedule.
For private-practice surgeons who own their schedule, the math compounds. A freed OR slot can mean an additional case, which matters most in plastic, cosmetic, and outpatient surgery settings where increased capacity drives revenue.
The overall ROI depends on device cost, case volume, and how consistently closure time drops in your specific case mix.
When Is Sutureless Skin Closure Not the Right Choice?
Sutureless skin closure isn't the right choice when wound conditions fall outside the narrow tolerances these methods are designed for. Contamination, deep tissue involvement, and high mechanical load are the three factors that most often push a case back to traditional suturing.
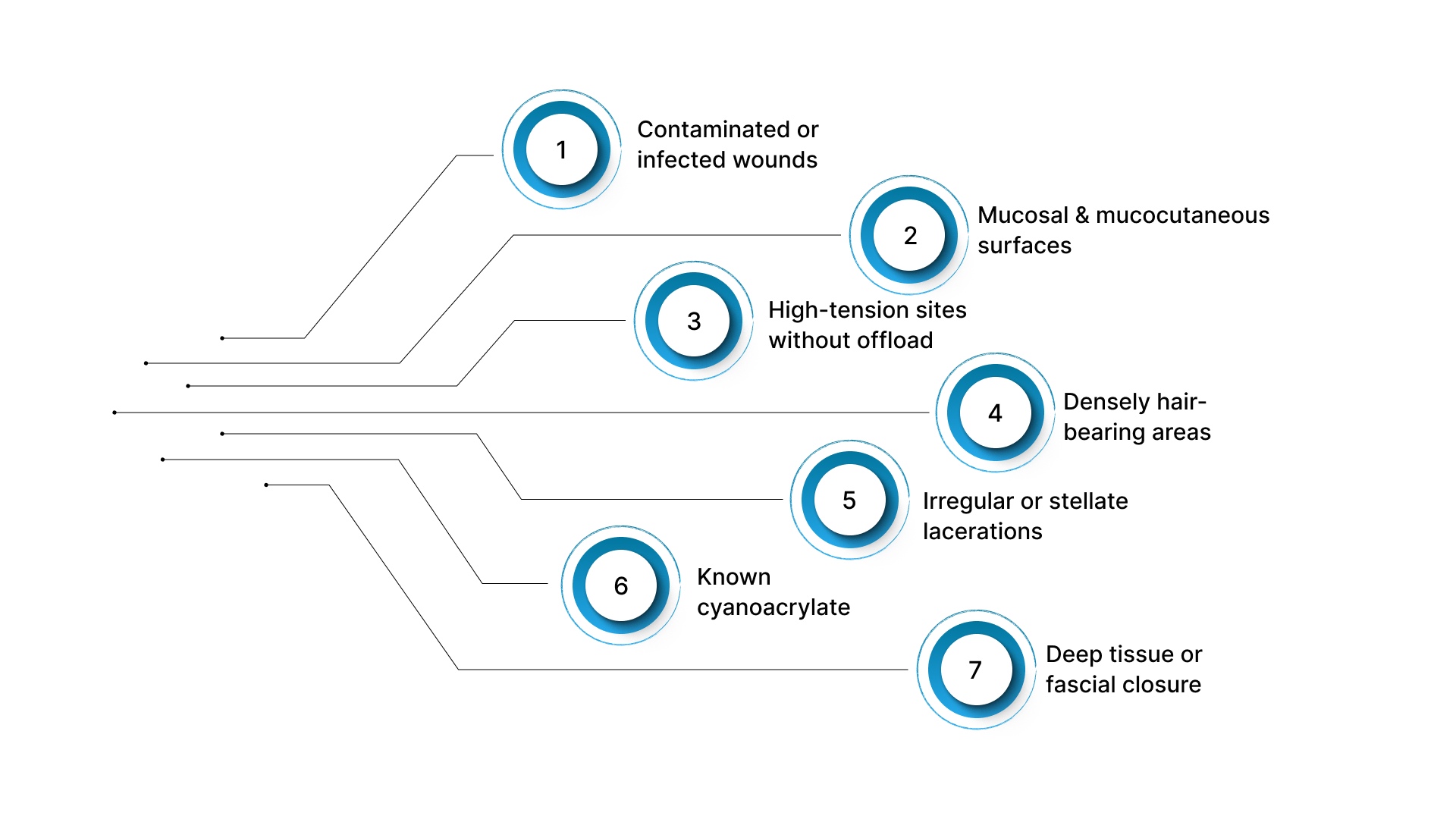
Here are the main exclusions:
- Contaminated or infected wounds: Tissue adhesives, strips, and zipper devices aren't appropriate for dirty, infected, gangrenous, or actively bleeding wounds.
- Mucosal and mucocutaneous surfaces: Cyanoacrylate adhesives and most surface closures fail on mucosal tissue, so these sites need suture.
- High-tension sites without offload: Joints, scalp, and other mobile areas need deep subcuticular support before any surface adhesive or strip is applied.
- Densely hair-bearing areas: Adhesion drops sharply on hair-bearing skin, which limits strips and zippers.
- Irregular or stellate lacerations: Jagged edges don't approximate cleanly under surface devices and typically need sutured repair.
- Known cyanoacrylate or formaldehyde sensitivity: Prior contact dermatitis to these compounds rules out most tissue adhesives.
- Deep tissue or fascial closure: Surface sutureless methods don't replace deep-layer closure.
The takeaway for practicing surgeons is that sutureless methods expand your options but don't replace traditional closure across the board. Matching the method to the wound condition is what keeps outcomes predictable.
Final Thoughts
Sutureless skin closure has moved from a niche option to a practical set of methods with documented trade-offs on closure time, scar outcomes, and complication rates. Tissue adhesives, adhesive strips, zipper devices, and bioabsorbable subcuticular staplers each earn their place in the closure toolkit, and the evidence base is now strong enough to choose on data, not habit.
A quick audit of your own case mix usually points to the right starting move. Note where closure time eats OR capacity, where scar complaints come back in clinic, and where staple removals crowd your follow-up schedule. That's often where a method change matters most.
SubQ It! brings bioabsorbable subcuticular stapling to both very small laparoscopic port sites and incisions up to 25 cm, with the SU-10 and SU-25 covering most case profiles surgeons run into. Every week on older closure methods is another week of avoidable OR minutes and return visits on your schedule. Contact us today for a custom quote tailored to your case volume.
FAQs
1. Can Patients Shower After Sutureless Closure?
Most tissue adhesives tolerate brief, gentle showering within a few hours of application, though soaking or scrubbing should be avoided until the adhesive sheds. For adhesive strips and zipper devices, guidance depends on the specific product, so surgeons should confirm instructions with each case.
2. How Common Are Allergic Reactions to Tissue Adhesives?
Allergic contact dermatitis to cyanoacrylate adhesives has been reported across a wide range in the literature. Known sensitivity to cyanoacrylate or formaldehyde is a contraindication, and a brief patient history before application helps screen for risk.
3. Do Bioabsorbable Staples Need Any Aftercare?
Bioabsorbable subcuticular staples don't require removal and generally need only standard incision-site care. Patients follow the usual instructions for keeping the area clean and watching for signs of infection, with no separate visit for hardware removal.
4. Can Sutureless Methods Be Used on Longer Surgical Incisions?
Yes, some specialized bioabsorbable subcuticular staplers are designed to handle longer incisions up to 25 cm. Tissue adhesives, strips, and zipper devices are generally better suited to shorter wounds or used as adjuncts to deeper suture support on longer closures.
5. How Does Sutureless Closure Affect Infection Risk?
Published data on absorbable subcuticular stapling in mastectomy showed infection rates statistically indistinguishable from hand-sewn suture. Surface sutureless methods perform comparably on clean wounds, but contaminated or infected wounds still need traditional suturing.
6. What Role Does Deep Tissue Closure Play With Sutureless Methods?
Sutureless skin closure methods approximate skin edges only. Deeper layers, including fascia and subcutaneous tissue, still need appropriate closure using absorbable suture or other techniques, regardless of which surface method is chosen.