Tissue adhesives can save up to 12 minutes per incision compared to subcuticular sutures. That's real OR time back on every case. The catch is that not every surgical glue name on the market fits every wound.
A cyanoacrylate-based adhesive built for skin closure won't do the same job as a fibrin sealant designed for internal hemostasis. Picking the wrong one for a given wound can affect healing time, cosmetic outcome, and complication risk.
This guide covers every surgical glue name by chemical family, clinical use, and named product. It also shows where adhesives reach their limits and which closure alternatives work for the incisions that glue can't handle.
Key Takeaways
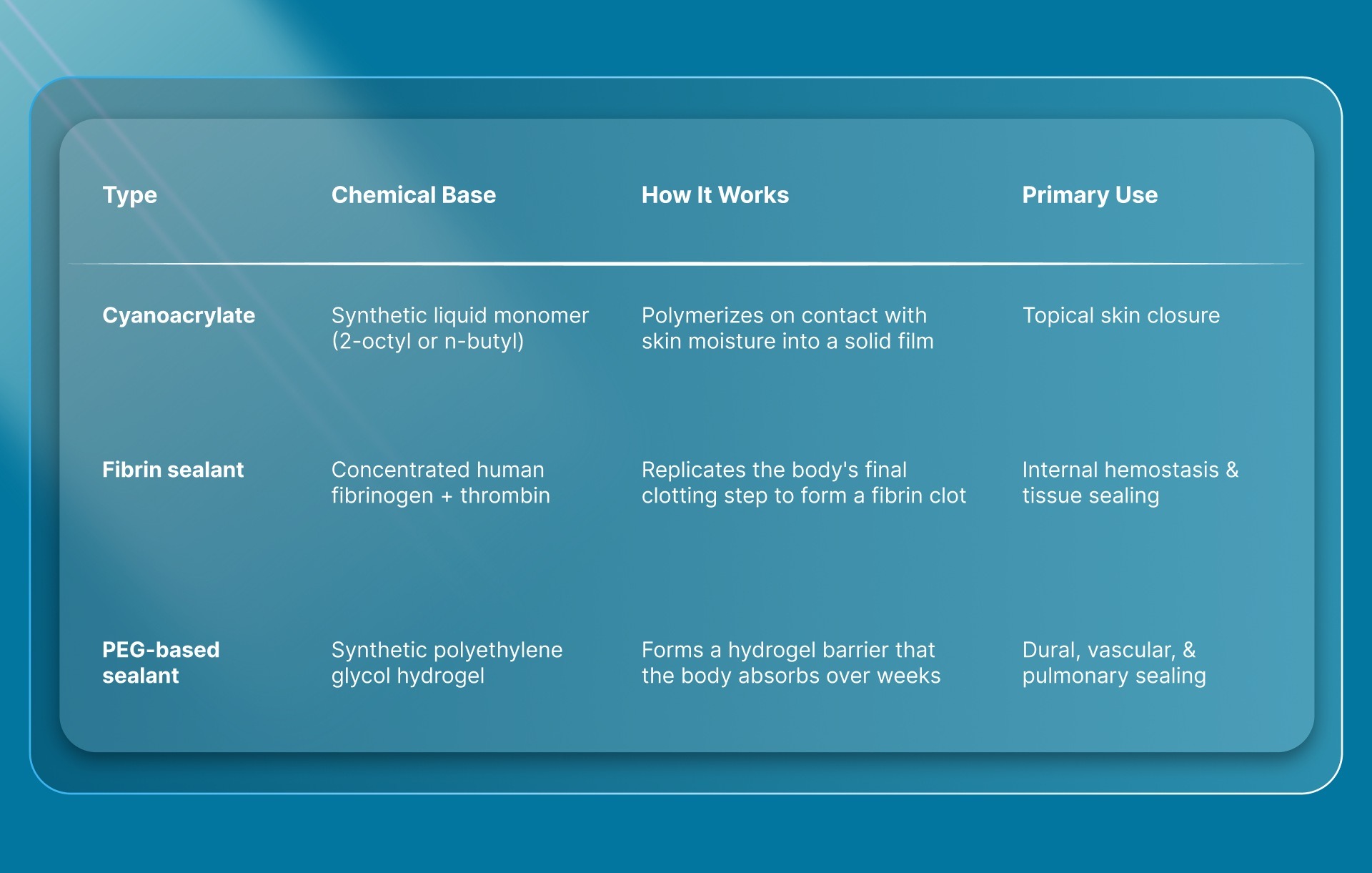
- Surgical glues fall into three chemical families, each designed for different clinical scenarios: cyanoacrylates for skin, fibrin sealants for internal hemostasis, and polyethylene glycol (PEG)-based polymers for dural and vascular sealing.
- 2-octyl cyanoacrylate products like Dermabond and SurgiSeal are the most widely used topical adhesives, forming a flexible, waterproof film that detaches on its own in 5 to 10 days.
- Cyanoacrylate adhesives close wounds faster than sutures but show better cosmetic results only in the first month; after three months, sutures tend to produce superior outcomes on face and neck wounds.
- Surgical glue isn't appropriate for high-tension, deep, or contaminated wounds, and reported skin reaction rates to 2-octyl cyanoacrylate range from 0.5% to 14% across published studies.
- For incisions where adhesive alone isn't strong enough, bioabsorbable subcutaneous staples offer a no-removal alternative that works on wounds up to 25 cm long.
What Is Surgical Glue?
Surgical glue is a liquid tissue adhesive applied to wound edges to hold them together while healing takes place. It's an alternative to sutures and staples for specific wound types, particularly low-tension skin incisions and small lacerations.
The most common type, 2-octyl cyanoacrylate, works by hardening into a thin, flexible film within seconds of touching the moisture on the skin surface. That film acts as both a wound closure and a waterproof protective barrier. It naturally detaches in 5 to 10 days without any follow-up visit for removal.
A practical example is a surgeon closing a small trocar site after a laparoscopic cholecystectomy. Instead of placing sutures, a thin layer of adhesive skin closure goes over the approximated wound edges and sets almost immediately. The patient leaves with a sealed incision and no need for suture removal down the line.
What Are the Main Types of Surgical Glue?
Surgical glues fall into three chemical families, and each one serves a different purpose in the OR. Knowing which family a product belongs to tells you immediately where it fits clinically.
Each family has practical nuances that affect product selection.
Cyanoacrylate-Based Adhesives
The two subtypes that matter clinically are 2-octyl cyanoacrylate and n-butyl cyanoacrylate. Both are long-chain variants that degrade slowly and cause less tissue irritation than short-chain types like methyl and ethyl cyanoacrylate. Short-chain variants release formaldehyde during breakdown, which can trigger local inflammation. That's why they aren't used for skin closure in surgical settings.
2-octyl cyanoacrylate produces a more flexible film and is the standard for most topical applications. N-butyl cyanoacrylate sets faster and works well for smaller wounds, but it's more rigid once polymerized.
Fibrin Sealants
Fibrin sealants are two-component systems made from concentrated human fibrinogen and thrombin. When the two mix on the tissue surface, thrombin converts fibrinogen into a stable fibrin clot, replicating the last step of the body's coagulation process.
They're used internally for hemostasis during procedures involving the liver, spleen, cardiovascular system, and other vascularized tissue. They also attach skin grafts and seal tissue layers during abdominal wound closure.
Polyethylene Glycol (PEG)-Based Sealants
PEG-based sealants are fully synthetic. They don't rely on human blood products, which removes the plasma-sourcing considerations that come with fibrin sealants.
Neurosurgeons use them to prevent cerebrospinal fluid leaks after posterior fossa and spinal procedures. They're also applied in vascular and thoracic cases to reinforce suture lines. The body absorbs the hydrogel over time.
What Are the Most Common Surgical Glue Names?
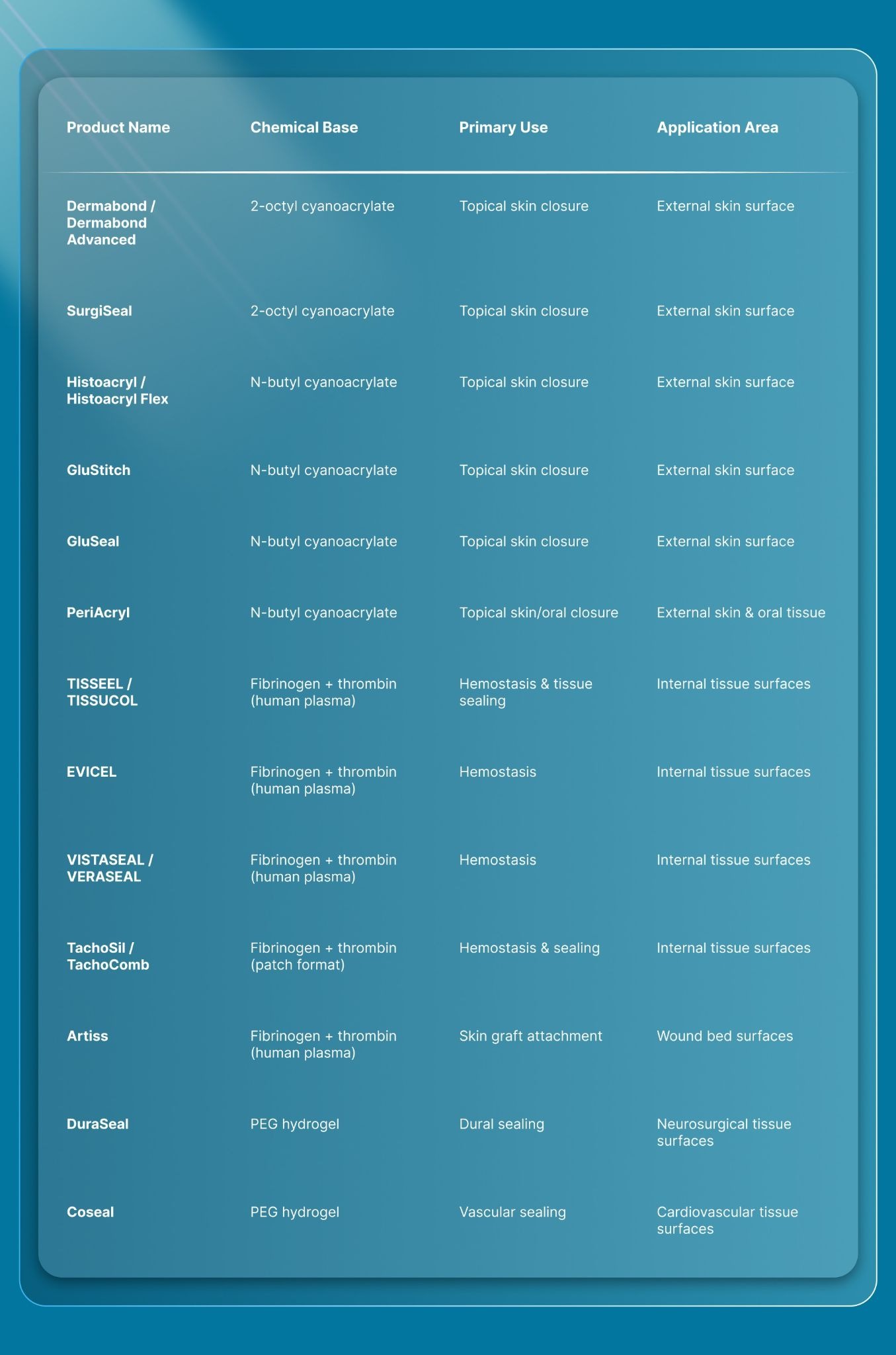
Here’s a quick overview of all major surgical glue names, mapped to their chemical bases, primary clinical uses, and application areas:
Each category has practical differences that matter when you're choosing between products.
Topical Cyanoacrylate Products
Dermabond and SurgiSeal are both 2-octyl cyanoacrylate formulations and are the most commonly referenced surgical glue brands in skin closure discussions. They form a flexible film that handles mild wound movement without cracking, which makes them a practical fit for facial lacerations and low-tension surgical incisions.
N-butyl cyanoacrylate products like Histoacryl, GluStitch, and GluSeal set faster and produce a slightly more rigid bond. They work well for smaller wounds where flexibility is less of a concern. PeriAcryl is often used in oral and dental applications because of its fast polymerization time on moist mucosal tissue. The choice between 2-octyl and n-butyl comes down to incision size, wound tension, and how much flexibility the closure site needs.
Internal Fibrin Sealant Products
TISSEEL is the most widely referenced fibrin sealant in published literature and clinical practice. EVICEL and VISTASEAL serve similar hemostatic roles with slightly different formulations. All three are liquid systems that require mixing two components at the point of use.
TachoSil takes a different delivery approach. It's a collagen patch pre-coated with fibrinogen and thrombin, which makes it easier to apply directly onto a bleeding tissue surface during surgery. Artiss is formulated specifically for attaching skin grafts, with a slower-setting thrombin concentration that gives the surgeon more working time to position the graft before the clot forms.
Synthetic PEG-Based Sealant Products
DuraSeal is the most recognized PEG-based surgical glue name. It's used primarily in neurosurgery to seal the dura after cranial and spinal procedures, where even a small cerebrospinal fluid leak can lead to complications like meningitis or pseudomeningocele. Coseal serves a similar sealing function in cardiovascular surgery, reinforcing suture lines along vascular grafts and anastomoses.
Both products are fully synthetic, which avoids the risk of blood-borne pathogen transmission associated with plasma-derived fibrin sealants. The body absorbs the hydrogel material over a period of weeks.
A 2025 review of biocompatible surgical adhesives noted that no single adhesive currently satisfies every surgical requirement, including biodegradability, strong wet-tissue bonding, and suitability across all wound types. That reality is what makes knowing the full product range and the wound closure device companies behind them so important.
How Is Surgical Glue Applied in the OR?
Topical cyanoacrylate adhesives follow a specific application sequence. Getting this right is what separates a clean closure from one that fails early.
- Approximate the wound edges. The incision or laceration edges need to be clean, dry, and held together before any adhesive touches the skin. Surgical glue doesn't pull wound edges together on its own. It only holds them in position.
- Apply thin layers. The adhesive goes on in thin, even coats across the wound surface. Pooling the liquid in one spot creates a thick, brittle mass that's more likely to crack or peel. Most clinical references recommend two to three passes.
- Allow polymerization. The monomer hardens within seconds on contact with skin moisture. The full bond strength builds over the first two to three minutes. Avoid touching or manipulating the wound during this window.
- Leave the barrier intact. Once set, the adhesive film acts as a waterproof dressing. No topical antibiotics or other medications should be placed over it, as they can weaken the adhesive barrier.
The polymerized film detaches naturally in 5 to 10 days as the outer skin layer regenerates underneath. There's no scheduled removal and no follow-up visit needed for the closure itself.
Adhesive application works best on specific wound profiles. When the wound falls outside those parameters, other types of skin closure are worth considering.
When Should Surgeons Choose Surgical Glue Over Other Closure Methods?
Surgical glue works best on clean, dry, low-tension wounds where the skin edges come together easily without significant pull. For anything outside that profile, sutures, staples, or bioabsorbable alternatives are worth considering.

Each method fills a different clinical niche. Here's how adhesive compares against the other three in practice.
Surgical Glue vs. Sutures
Cyanoacrylate adhesives close wounds faster than sutures. One 2024 randomized trial in ear surgery patients found that octyl-2-cyanoacrylate reduced average skin closure time by 12 minutes per incision compared to subcuticular sutures.
The cosmetic trade-off is time-dependent. A 2023 meta-analysis of 18 randomized controlled trials (1,020 patients) found that adhesives delivered better physician-rated cosmetic scores than sutures in the first month of healing on face and neck wounds. After three months and up to one year, sutures showed superior cosmetic results. Complication rates were similar between the two groups.
Surgical Glue vs. Metal Staples
Metal staples are fast to place and handle higher-tension closures than adhesive. They're common in orthopedic, abdominal, and scalp procedures. The downside is cosmetic and logistical. Metal staples sit on the skin surface, leave railroad-track scarring, and require removal in 7 to 10 days.
Surgical glue avoids both issues. It doesn't pierce the skin and doesn't need removal. It also can't match the holding strength of staples on skin closure under tension, which limits its use on longer or more active wound sites.
Surgical Glue vs. Bioabsorbable Staples
Bioabsorbable staples are placed subcutaneously (under the skin surface), dissolve on their own after healing, and don't require a removal visit.

SubQ It! is a bioabsorbable wound closure system that uses vertical dermal fasteners placed beneath the skin. The SubQ It! SU-25 variant closes incisions up to 25 cm, and it's the only product in its category that also handles very small laparoscopic trocar sites with the SubQ It! SU-10. SubQ It! SU-25 saves approximately 25 minutes of OR time per case compared to manual suture closure, with no railroad-track scarring.
Surgical glue is ideal for small, superficial, low-tension closures. Bioabsorbable staples serve the incisions where adhesive alone wouldn't hold and where the surgeon wants to avoid the scarring and removal visit that come with metal staples.
What Are the Limitations of Surgical Glue?
Cyanoacrylate adhesives work well within a specific wound profile. Outside that range, outcomes decline.
- Wound tension: Adhesive bonds aren't strong enough for incisions under significant pull or movement. High-tension sites like joints, the trunk during active movement, and weight-bearing areas are better served by sutures or staples.
- Wound depth: Surgical glue bonds the skin surface only. It can't replace deep-layer closure with absorbable sutures or fascial repair.
- Contaminated wounds: Cyanoacrylate is not indicated for infected or contaminated wounds. The adhesive traps bacteria beneath the seal, which can worsen infection.
- Skin reactions: Allergic contact dermatitis to 2-octyl cyanoacrylate is documented. A 2025 systematic review combining published literature with 609 adverse event reports found reaction rates ranging from 0.5% to 14% across studies. Symptoms typically appear around 10 days after application and include swelling, redness, and blistering at the wound site.
- Incision length: Maintaining consistent edge approximation with adhesive gets harder as the incision grows. For longer wounds, a closure method with mechanical holding strength is more reliable.
For closures that fall outside this wound profile, alternatives like bioabsorbable wound closure systems and subcuticular skin closure methods serve the incision sizes and tension levels that adhesive can't.
Final Thoughts
Surgical glue names span three chemical families, each built for a specific surgical role. Cyanoacrylates close surface skin wounds. Fibrin sealants control internal bleeding. PEG-based polymers seal dural and vascular tissue. Knowing which product name belongs to which category makes it easier to match the adhesive to the wound.
The practical next step is straightforward. When the wound is clean, dry, low-tension, and on the skin surface, a cyanoacrylate adhesive is a strong option. When the incision is longer, under more tension, or in a location where cosmetic outcome matters long-term, consider a closure method with mechanical strength and no need for a return visit.
SubQ It! fills that space for incisions up to 25 cm. Its bioabsorbable dermal fasteners close subcutaneously, dissolve after healing, and save up to 25 minutes of OR time per case. For private practice surgeons, that time savings translates to roughly $6,000 in additional revenue per case. Contact us today to request a custom quote and see how it fits into your closure workflow.
FAQs
1. Is Surgical Glue the Same as Super Glue?
No, they're chemically related but not interchangeable. Medical-grade cyanoacrylates like 2-octyl cyanoacrylate are formulated specifically for use on human skin, with longer alkyl chains that reduce tissue irritation and the release of toxic byproducts during degradation.
2. How Long Does Surgical Glue Take to Dry?
Most cyanoacrylate tissue adhesives harden within seconds of contact with skin moisture. Full bond strength develops over the first two to three minutes, which is why the wound shouldn't be manipulated during that time.
3. Can Surgical Glue Be Used on Deep Wounds?
No, topical cyanoacrylate adhesives only bond the outer skin surface. Deep wounds that involve fascia, muscle, or subcutaneous tissue need internal closure with absorbable sutures before any surface adhesive is applied.
4. Does Surgical Glue Leave a Scar?
Yes, any wound closure method leaves some degree of scarring. Surgical glue tends to produce narrower scars in the short term, but long-term cosmetic outcomes depend on wound location, tension, and individual healing response.
5. How Long Does Surgical Glue Stay on the Skin?
The polymerized film typically stays in place for 5 to 10 days. It detaches naturally as the outer skin layer regenerates underneath. Patients should not pick at or peel the adhesive, as doing so can reopen the wound.
6. What Happens if Surgical Glue Gets Inside a Wound?
Cyanoacrylate adhesive placed inside a wound rather than on the surface can delay healing and increase the risk of infection. It's designed for topical use only, applied over wound edges that are already held together.