Re-selecting a surgical needle or working against tissue drag adds minutes to OR time. Across a full surgical day, those minutes extend anesthesia, delay subsequent cases, and increase the cost per procedure.
Selecting the right needle type and curvature for the tissue reduces pass count and speeds up closure. It also lowers sharps exposure, which matters given that 41.5% of OR professionals have reported at least one sharps injury over their career.
This guide covers surgical needle types, curvature, sizing, handling, and when a needle-free skin closure option is clinically appropriate.
Key Takeaways
- A surgical needle has three parts, and the point geometry (taper, cutting, blunt, or spatula) should match the tissue you're closing.
- Reverse cutting needles are the go-to for skin because their blade sits on the outer curve, reducing the risk of suture tear-through.
- Taper point needles part tissue fibers instead of slicing them, making them well-suited for soft tissue like bowel, vessels, and peritoneum.
- The 3/8-circle curve is the standard for most skin work, while a 1/2-circle works better in deep or tight spaces like the pelvis.
- Clamp the needle holder about one-third back from the tip to prevent bending and keep your arc controlled.
What Is a Surgical Needle?
A surgical needle is a sterile, stainless steel instrument designed to carry suture thread through tissue. Every needle is built around three zones. The tip pierces the tissue, the body (or shaft) is where the needle holder grips, and the swage is where the suture attaches to the metal.
Modern needles are swaged, which means the suture is bonded directly onto the needle at the factory. This removes the old threaded-eye design, where a doubled thread had to pass through the tissue and created a wider channel. A swaged needle pulls a single strand, so the hole in the tissue stays closer to the actual suture diameter.
The wrong needle for a given tissue is noticeable on the first pass. A cutting needle in the bowel wall slices fibers that should be parted gently. A taper needle in thick skin resists every pass. The right match between needle and tissue is what keeps needle driver suturing smooth and needle stitches consistent.
What Are the Main Types of Surgical Needles?
Surgical needles fall into four main categories based on their point geometry. Each one is built for a specific tissue type. Picking the right point type reduces tissue trauma, holds the suture more securely, and speeds up your closure.
Here’s a detailed breakdown of each type:
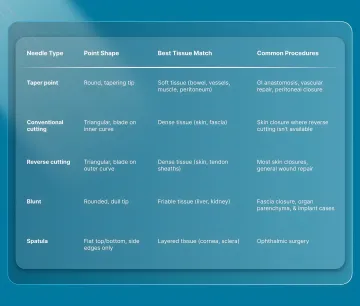
1. Taper Point Needles
Taper point needles have a round, cylindrical body that narrows gradually to a fine tip. There are no blade edges anywhere on the needle. Instead of slicing, the tip pushes tissue fibers apart and lets them close snugly around the suture behind the needle. That natural seal is why tapers are well-matched for soft tissue like intestinal walls, blood vessels, muscle, and peritoneum.
In a 2025 lab study on an artificial skin model, taper point needles held up to 4.07 N of force before the suture tore through, compared to 3.75 N for reverse cutting and 3.26 N for conventional cutting. Both needle shape and thread diameter independently affected how well the suture held in tissue.
2. Cutting Needles
Cutting needles have a triangular cross-section with sharpened edges, built for dense, resistant tissue like skin and fascia. They come in two subtypes. Conventional cutting needles place the blade along the inner curve. Reverse cutting needles shift the blade to the outer curve.
Most surgeons reach for reverse cutting when closing skin, because the flat inner face rests against the wound margin and is less likely to let the suture saw through the tissue edge.
A related 2025 study measured the actual force needed to pass taper and reverse cutting needles through human abdominal skin. The difference between the two was not clinically meaningful at any gauge size tested. That finding challenges the common assumption that cutting geometry always enters skin far more easily than taper geometry.
3. Blunt Needles
Blunt needles have a rounded, dull tip. They're designed for tissue that tears easily (friable tissue), like liver and kidney parenchyma. The blunt tip pushes through without slicing, which reduces the risk of accidental organ damage.
Blunt needles also carry a significant safety benefit. A 2024 pooled analysis of 14 randomized trials found that blunt-tipped needles roughly halved glove puncture risk and percutaneous injury risk compared to sharp needles. Surgeons did report that blunt needles were harder to handle, but the safety advantage was significant enough for the authors to recommend routine adoption, especially during closures involving implants.
4. Spatula Needles
Spatula needles are flat on both the top and bottom, with sharp edges only on the sides. They're built specifically for ophthalmic procedures, where the surgeon needs to separate tissue layers without piercing through the full thickness. You won't come across them outside eye surgery, but they're the standard in that specialty.
Each needle type exists because tissue types differ. Matching the point geometry to the tissue is the single fastest way to improve suture hold and reduce trauma. For skin closure specifically, surgeons are also now moving toward modern options that skip the suture device entirely.
Bioabsorbable subcutaneous fasteners from SubQ It! place closures beneath the skin without any external needle passes, which removes the scarring pattern that non-absorbable sutures and metal staples leave behind.
How Does Needle Curvature Affect Your Closure?
The curvature of a surgical needle determines how easily you can arc through tissue at a given depth. The right curve lets you complete each pass in one controlled motion. However, the wrong one forces awkward wrist angles, repeated attempts, or incomplete tissue bites.
Curved needles are measured by the fraction of a full circle they trace. Here's how each curvature maps to clinical use.
Here's a closer look at each option and when it fits:
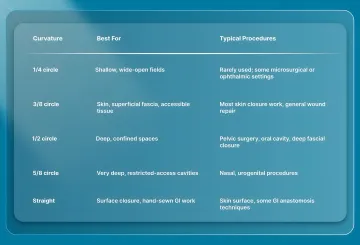
1/4 Circle Needles
The 1/4 circle traces the shallowest arc of any curved needle. It needs a wide, open operative field to complete the pass, which limits its use to microsurgical and select ophthalmic settings. Most general surgical trays won't stock this curvature.
3/8 Circle Needles
The 3/8 circle is the default for most skin work and any tissue accessible from above. It gives a wide, sweeping arc that's easy to follow with a wrist rotation. Because the curve is relatively shallow, the entry and exit points stay visible throughout the pass.
Closing a wound on the extremities, torso, or scalp with direct surface access typically calls for a 3/8 circle paired with a reverse cutting tip. It's also the most common curvature stocked on general surgical trays.
1/2 Circle Needles
A 1/2 circle needle traces a deeper arc, which lets it reach tissue at the bottom of a confined space without needing extra room to maneuver. Pelvic procedures, deep abdominal subcuticular closures, and oral cavity work all benefit from this tighter curve.
The trade-off is that a 1/2 circle requires more wrist pronation and can be harder to control in shallow wounds. It's most useful when a 3/8 circle can't complete the arc in the available space.
5/8 Circle Needles
The 5/8 circle has the deepest arc of any standard curved needle. It's reserved for very deep, restricted-access cavities like nasal and urogenital procedures, where the surgeon needs to place sutures with minimal wrist clearance. Like the 1/4 circle, it's a specialty curvature that won't appear on most general trays.
Straight Needles
Straight needles don't require a needle holder at all in some cases. They're used for surface skin closure and for certain hand-sewn gastrointestinal (GI) anastomosis techniques where the surgeon needs direct, linear passes through tissue. They're uncommon in most OR settings, but they serve a specific role when the tissue is accessible and the closure is linear.
Picking the right curvature alongside the right point type is what makes each pass efficient. When those two choices are matched to the tissue and the depth, your absorbable sutures sit exactly where you placed them.
How Do You Pick the Right Surgical Needle Size?
The best needle size is the smallest one that securely holds the suture and matches the depth of the tissue. A needle that's too large creates a wider tissue channel than necessary. One that's too small won't carry the suture through dense tissue or may bend under the force.
Surgical needle size is measured in millimeters, from the tip to the swage end. The needle size generally tracks with the suture gauge, so the two decisions go together.
Here are the key sizing principles to consider while selecting the right surgical needle:
- Fine sutures, small needles: Finer suture gauges pair with smaller needles for delicate tissue like vessels and skin edges on the face.
- Heavy sutures, larger needles: Heavier suture gauges pair with larger needles for fascia and thick abdominal skin.
- Depth and access: In a confined space, the needle needs to be small enough to complete its arc without contacting surrounding structures. A deep skin stapler vs. suture decision on the abdomen calls for a larger needle than a superficial forearm closure.
- When in doubt, size down: A smaller needle causes less tissue displacement and still carries the suture if the needle gauge and suture diameter are properly matched.
Deliberate sizing consistently produces better suture skin closure outcomes than defaulting to whatever was pre-loaded on the tray.
What Are the Best Practices for Handling Surgical Needles?
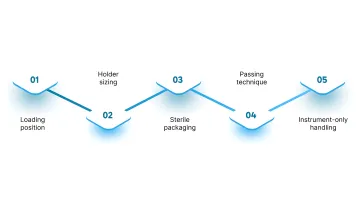
Surgical needles perform best when loaded and passed with a consistent technique. Proper handling protects the needle's geometry, keeps the arc predictable, and reduces injury risk for the entire team. Here are the key handling principles and best practices to follow:
- Loading position: Clamp the needle holder about one-third of the way back from the tip, at the junction of the middle and rear third of the body. This position provides the best arc control without risking bending or breakage.
- Holder sizing: Match the needle holder to the needle. A holder that's too large can flatten the needle's curvature. One that's too small lets the needle spin in the jaws.
- Sterile packaging: Keep the needle sealed until the moment of use.
- Passing technique: Secure the needle in the holder and present it handle-first. The receiving hand grips the box lock while the needle points away from both people.
- Instrument-only handling: Fingers should never contact the needle directly. All loading, repositioning, and passing should happen through instruments.
These habits are especially relevant during long closures, where fatigue increases the chance of a missed grip or uncontrolled pass.
How Can You Reduce Sharps Injuries from Surgical Needles?
Sharps injuries remain one of the most common risks in the OR, and suture needles are a leading cause. According to a study tracking 106 surgeons, found that 65% of suture needle injuries happened during closures on incisions exceeding 10 cm. Limited visibility was the top contributing factor in 70% of cases.
Here’s how you can reduce injuries from surgical needles:
- Neutral-zone passing: Place the needle in a designated tray or magnetic pad between handoffs instead of passing hand to hand. This removes the direct-transfer risk that accounts for nearly a quarter of OR sharps injuries.
- Blunt needles for fascia: When closing fascia or tissue around implants, blunt-tipped needles reduce the risk of glove puncture and percutaneous injury compared to sharp needles.
- Fewer needle passes: Any closure method that reduces the total number of needle passes in a case reduces cumulative exposure for the entire surgical team.
Reducing needle time during skin closure is one direct way to lower that exposure. However, alternatives like bioabsorbable subcutaneous fasteners can also help close the skin without external needle passes, removing the needle-handling step entirely for that portion of the procedure.
What Are There Skin Closure Options That Don't Require a Surgical Needle?
For skin closure specifically, a surgical needle isn't always the only option. Adhesive strips, tissue glue, metal staples, and bioabsorbable subcutaneous fasteners can all close skin without a needle-and-thread technique.
Adhesive skin closure strips work well for superficial, low-tension wounds. Tissue glue (cyanoacrylate) bonds skin edges together and is common for small lacerations and pediatric closures. Metal staples are fast but sit on the skin surface, require a removal visit, and leave the railroad-track scarring pattern from external puncture marks.

SubQ It! takes a different approach. Its bioabsorbable dermal fasteners are placed beneath the skin (subcutaneously), so they never pierce the outer surface. They dissolve naturally after healing is complete, which removes the need for a return visit for removal.
For small and laparoscopic incisions, SubQ It! SU-10 places 10 fasteners and closes incisions up to 10 cm. For longer incisions up to 25 cm, SubQ It! SU-25 provides 25 fasteners and saves approximately 25 minutes of OR time compared to manual sutureless skin closure or traditional needle-and-thread.
Time savings especially matter in a private practice or ambulatory surgery center, where 25 minutes per case can change the number of patients you see in a day. The fasteners also leave only the original incision line behind, with no external puncture marks. For surgeons looking for an alternative to suture skin closure that's both fast and cosmetically clean, it's worth considering.
Final Thoughts
Surgical needle selection is a tissue-specific, procedure-specific decision. The point type, curvature, and size all need to match the tissue you're closing and the space you're working in. Getting those three choices right reduces trauma, improves suture hold, and keeps your OR moving.
A practical next step is reviewing whether the default needle setup on your trays matches the tissue profile of your most common cases. A different point type or curvature may serve certain procedures better. For skin closure, it's also worth evaluating whether every incision on a given surgical day requires a needle-and-thread approach.
SubQ It! offers a bioabsorbable, subcutaneous skin closure system that closes incisions up to 25 cm without external needle passes, staple removal visits, or railroad-track scarring. Surgeons who adopt it early reclaim OR minutes on every case. Contact us today for a custom quote and see how it fits into your closure workflow.
FAQs
1. Can You Reuse a Surgical Needle?
No, surgical needles are single-use, sterile instruments. Reusing them increases infection risk and causes tissue trauma because the tip dulls after one pass through tissue.
2. What Is the Difference Between a Taper and a Cutting Needle?
A taper needle has a smooth, round body that pushes tissue fibers apart without slicing. A cutting needle has a triangular cross-section with sharp edges built for dense tissue like skin and fascia.
3. Why Are Most Surgical Needles Curved?
Curved needles let the surgeon arc through tissue in a controlled, rotational wrist motion. Curved designs also make it easier to place sutures in deep or confined spaces where a straight pass would be impractical.
4. What Material Are Surgical Needles Made Of?
Most surgical needles are made from corrosion-resistant stainless steel. Many are coated with silicone to reduce friction and make the needle pass through tissue more smoothly.
5. How Do You Dispose of a Surgical Needle Safely?
Place used surgical needles directly into a puncture-resistant sharps container at the point of use. Never recap, bend, or pass a bare needle by hand after use.
6. What Is a Swaged Needle?
A swaged needle has the suture permanently bonded to the needle at the factory, creating a smooth junction. This design creates a smaller channel through tissue than older threaded-eye needles that carried a doubled strand.